Abstract
Multiple myeloma (MM) is the second most frequent hematological disease. Two-thirds of newly diagnosed MM patients are more than 65 years of age. Elsewhere in this issue, McCarthy et al discuss the treatment of transplantation candidates; this chapter focuses on the data available concerning therapy for non-transplantation-eligible MM patients. Treatment goals for these non-transplantation-eligible patients should be to prolong survival by achieving the best possible response while ensuring quality of life. Until recently, treatment options were limited to alkylators, but new up-front treatment combinations based on novel agents (proteasome inhibitors and immunomodulatory drugs) plus alkylating agents have significantly improved outcomes. Other nonalkylator induction regimens are also available and provide a novel backbone that may be combined with novel second- and third-generation drugs. Phase 3 data indicate that maintenance therapy or prolonged treatment in elderly patients also improves the quality and duration of clinical responses, extending time to progression and progression-free survival; however, the optimal scheme, appropriate doses, and duration of long-term therapy have not yet been fully determined. The potential for novel treatment regimens to improve the adverse prognosis associated with high-risk cytogenetic profiles also requires further research. In summary, although we have probably doubled the survival of elderly patients, this group requires close monitoring and individualized, dose-modified regimens to improve tolerability and treatment efficacy while maintaining their quality of life.
Introduction
Multiple myeloma (MM) is a fatal cell disease that accounts for 1% of all cancers and 10% of hematological malignancies. It primarily affects older individuals; the median age at diagnosis is 70 years and two-thirds of MM patients are more than 65 years of age when they are first diagnosed. The increased life expectancy of the general population means that an increase in the number of elderly MM patients is expected over time. The outcome of MM has significantly improved in the last decade because myeloma treatment is developing rapidly.1,2 The main benefit was first accrued by young patients, who benefited from the introduction of high-dose therapy followed by autologous stem cell transplantation (HDT-ASCT) up-front and the use of novel agents as rescue therapy, although only a marginal change was observed in patients older than 65 years. However, the availability of new frontline treatment regimens has extended the options also for non-transplantation-eligible MM patients. Due to the increased life expectancy of the general population and the improved survival arising from better antimyeloma drugs, the number of MM patients will increase substantially worldwide in the future.
Initial therapy for MM depends on eligibility for HDT-ASCT. Elsewhere in this issue, McCarthy et al discuss the treatment of transplantation candidates; this chapter focuses on the available data about therapy for non-transplantation-eligible MM patients. The role of novel therapies in patients with high-risk cytogenetic abnormalities and comorbidities for optimized disease control is also discussed. The ultimate objective is to provide an outline to help physicians choose and optimize treatment strategies for this patient population.
Can we go beyond complete response as a goal of therapy?
The introduction of new treatment options for non-transplantation-eligible patients has altered the goals of therapy. Prolongation of disease-free survival and overall survival (OS) remains the ultimate goal, but achieving prolonged treatment-free intervals and good quality of life have also become important aims, especially for elderly patients. In the era of MP (melphalan plus prednisone), the goal was to achieve partial response; in contrast, with the new agents, complete response (CR) has become the new goal, including in elderly patients. The role of CR has been evaluated in elderly patients. In a retrospective analysis of pooled data from 1175 patients with newly diagnosed MM treated with novel agents and MP, achieving CR was associated with improved progression-free survival (PFS) and OS.3 Moreover, upon using more sensitive parameters such as free light-chain and multiparameter flow cytometry to define the depth of response, the Spanish group's prospective analysis of elderly patients receiving novel agents showed that achieving an immunophenotypic response translated into better PFS compared with conventional CR or stringent CR.4 Therefore, monitoring treatment efficacy with highly sensitive techniques should also be an objective in the treatment of elderly patients, because this could help clinicians define the optimal level of response and individualize treatment intensity and duration while also taking into account the toxicity of the treatment.
Options for induction therapy
Alkylator-containing induction regimens
Melphalan was the first active alkylating agent used to treat MM patients, and MP was the standard of care for more than 30 years, although it yielded PRs in 40% to 60% of patients, <5% CRs, PFS of approximately 18 months, and OS of 2-3 years.5
Although it should no longer be considered the standard of care, MP has been the backbone for proteasome inhibitor and immunomodulatory drug combinations and is used as the comparator arm for the evaluation of novel agents in the treatment of elderly MM patients.
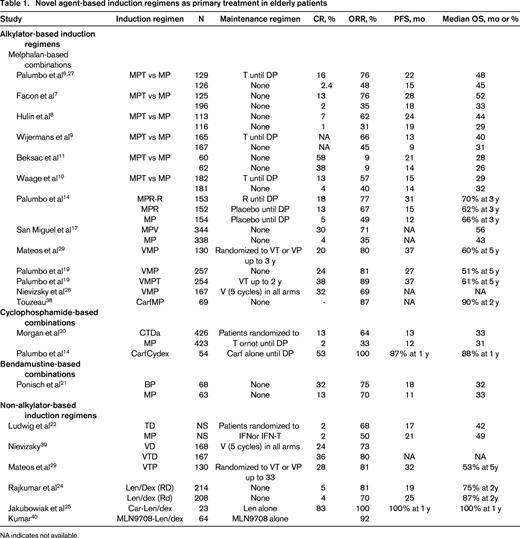
Six randomized trials compared the combination of MP plus thalidomide (MPT) with the standard MP.6-11 The PR rate was 42% to 76% versus 28% to 48% with MPT and MP, respectively, and PFS was 14 to 28 versus 10 to 19 months. In 3 of the 6 trials, the PFS advantage observed with MPT also translated into a significant OS advantage (37-52 vs 28-32 months), but this was not confirmed in the 3 other trials. A meta-analysis of pooled data from 1682 patients from the aforementioned 6 MPT trials showed that the addition of thalidomide to MP is associated with a significant improvement in PFS (5.4 months of benefit; hazard ratio [HR] = 0.67; 95% confidence interval, 0.55-0.80) and a nearly significant improvement in OS (6.6 months of benefit; HR = 0.82; 95% confidence interval, 0.66-1.02).12 These results indicate that the 3-drug combination is far superior to standard MP and support the use of MPT as one of the standards of care for elderly MM patients (Table 1). With respect to its toxicity, the median incidences of grade 3-4 peripheral neuropathy (PN) and venous thromboembolism (VTE) were 13% and 6%, respectively,13 meaning that antithrombotic prophylaxis is required when using MPT.
Lenalidomide instead of thalidomide in combination with MP and followed by maintenance with lenalidomide (MPR-R) has been compared with fixed duration regimens of MP and MPR (9 cycles) in a randomized placebo-controlled phase 3 trial (MM-015) in newly diagnosed elderly patients.14 Compared with MP, MPR induction treatment was associated with higher response rates (77% vs 50%) and greater CR rates (18% vs 5%). The most significant adverse events (AEs) observed with this combination were neutropenia (36% grade 4), thrombocytopenia (13% grade 4), and infections (15% grade 4). The median PFS did not differ significantly between the 2 induction regimens and the benefit of this combination mainly accrued from maintenance therapy. The results of the primary comparison of this study (MPR-R maintenance vs MP) are discussed in the section on maintenance treatment.
In the case of bortezomib, the randomized phase 3 VISTA trial compared the proteasome inhibitor bortezomib plus MP (VMP) with MP. VMP was superior to MP in ORR (71% vs 35%, P < .001), CR rates (30% vs 4%, P < .001), and in terms of time to progression (TTP; 24.0 vs 16.6 months, respectively; P < .001). From the first analysis with 16.3 months of follow-up15,16 until the last update with a median follow-up of 60 months,17 VMP showed a persistent significant benefit, with a 13.3-month increase in the median OS in the last analysis (HR = 0.695; P = .0004; median OS 56.4 vs 43.1 months; Table 1). However, the addition of bortezomib to the MP regimen also increased the rate of grade 3 or 4 AEs associated with treatment, particularly PN (14%) and gastrointestinal AEs (19%). Antiviral prophylaxis is required to prevent the reactivation of herpes virus. On the basis of these data, VMP has been recognized as a new standard of care for elderly untreated MM patients.
Despite the favorable clinical benefits of VMP, AEs are an important concern. The Spanish group investigated the VMP regimen but in a reduced-intensity bortezomib schedule based on the weekly administration of bortezomib; patients received the first cycle as a conventional twice-weekly dose and the other 5 cycles were administered as a weekly dose. After 6 cycles, the incidence of grade 3 or 4 PN dropped to 7%, with an ORR of 80% (20% CR)18 and, after maintenance therapy with VT or VP (see below), the PFS and OS were 37 and 60 months, respectively. The Italian group obtained similar results in a randomized trial comparing VMP (9 cycles) with VMPT, followed by maintenance therapy with VT. The schedule was initially based on the standard twice-weekly dose of bortezomib, but was subsequently amended to a weekly dose. The incidence of grade 3 or 4 PN in the VMP and VMPT weekly schemes was 5% and 8%, respectively. The addition of the 4 drugs to VMP (VMPT) plus maintenance with VT resulted in higher ORR and CR rates than obtained with VMP (89% vs 81% ORR and 38% vs 24% CR, respectively).19 The benefit of VT as maintenance will be discussed in the maintenance section.
Cyclophosphamide, another alkylating agent with proven efficacy in MM, has been evaluated in the Medical Research Council (MRC) Myeloma IX study, a randomized trial in elderly patients that compared the efficacy and safety of a regimen of cyclophosphamide, thalidomide, and attenuated dexamethasone (CTDa) compared with MP.20 CTDa produced a significant 2-fold improvement in overall response rates (64% CTDa vs 33% MP), although survival outcomes were not significantly different between the 2 regimens. CTDa was associated with higher rates of thromboembolic complications, PN, infection, and constipation than MP, indicating that adequate management of AEs is required to allow patients to continue the regimen and eventually benefit from the CTDa treatment. The same group is currently evaluating the same combination by replacing thalidomide with lenalidomide in a phase 3 trial.
More recently, bendamustine has been incorporated into the treatment armamentarium of MM. It has structural similarities with alkylating agents and purine analogs and is currently approved in Europe for the treatment of newly diagnosed MM patients who are not candidates for HDT-ASCT and who cannot receive thalidomide or bortezomib because they have a PN. The rationale for the approval was a randomized trial in which BP (bendamustine plus prednisone) proved to be superior to MP with respect to CR rate (32% vs 13%, P = .007), with a benefit in terms of time-to-treatment failure (14 months for BP vs 10 months for MP, P = .020), but without any benefit to OS.21 The toxicity profile was comparable and hematological toxicity and nauseas and vomiting were the most frequent AEs reported with BP. Bendamustine plus prednisone in combination with bortezomib is currently being evaluated in several pilot clinical trials.
Alkylating agents in combination with second-generation proteasome inhibitors are emerging as new therapeutic options also for newly diagnosed non-transplantation-eligible MM patients. In a pilot phase 1/2 trial, carfilzomib combined with MP (CMP) is yielding promising efficacy results (ORR of 92% and rate of very good partial response [VGPR] or better of 42%) with an acceptable toxicity profile and no grade 3-4 PN, providing the rationale for a randomized trial comparing CMP with VMP. The combination of carfilzomib plus cyclophosphamide and low-dose dexamethasone is being evaluated in a series of 53 newly diagnosed elderly MM patients, achieving ORR rates of 100%, including 53% CR and 22% stringent CR. No grade 3-4 PN was reported and tolerability was good. Ixazomib (MLN9708), an oral second-generation proteasome inhibitor, plus MP in a biweekly or weekly scheme is also currently undergoing a phase 1/2 clinical trial to evaluate the efficacy and safety of this combination (Table 1).
Non-alkylating-agent–containing induction regimens
Thalidomide and dexamethasone (TD) was approved in the United States in newly diagnosed MM patients on the basis of results from 2 randomized trials. TD was compared with MP in a cohort of elderly MM patients22 ; although it induced higher response rates than MP (68% vs 50%, P = .002), OS was significantly shorter with TD (41.5 vs 49.4 months, P = .024), and this was particularly evident in patients more than 75 years of age (20 vs 41 months). This paradoxical result arose from the higher frequency of non-disease-related deaths observed in the TD group during the first year. Therefore, TD in elderly patients is not a good option, unless patients receive reduced doses of both drugs.
The Spanish myeloma group evaluated the combination of thalidomide with a daily dose of 100 mg plus prednisone and bortezomib (VTP) in the same reduced-intensity bortezomib schedule mentioned in the previous section compared with VMP as induction therapy. After 6 cycles, the ORR was 81%, including 28% CR with 9% grade 3 or 4 PN.18
The change to the immunomodulatory drug lenalidomide in combination with dexamethasone (Len/Dex) proved to be superior to dexamethasone plus placebo in a randomized Southwest Oncology Group (SWOG) trial in newly diagnosed MM patients, including those more than 65 years of age.23 In this trial, Len/Dex was associated with an improved ORR and 12-month PFS but no OS benefit, probably due to the crossover design of this study. The dose of dexamethasone used in combination with lenalidomide is important with respect to the tolerability of the regimen, especially in elderly patients. A randomized, open-label ECOG study compared lenalidomide and high-dose dexamethasone (Len/Dex) with lenalidomide and low-dose dexamethasone (Len/dex) in newly diagnosed MM patients.24 Patients in this trial included elderly transplantation-ineligible patients as well as younger patients. Young patients were able to choose whether to proceed to ASCT after 4 treatment cycles. The Len/Dex regimen was associated with a higher ORR than Len/dex (79% vs 68%, P = .008), but the 1-year OS was superior for low-dose dexamethasone, although there were no differences at 3 years (Table 1). However, a survival benefit was observed with the low-dose regimen in patients more than 65 years of age, even when using a landmark analysis to eliminate the 5% of early deaths seen in the first 4 months of treatment. This difference was at least partially due to the greater toxicity of the high-dose dexamethasone (the incidence of grade 3 or 4 VTE events was 26% vs 12%; infections, 16% vs 9%; fatigue, 15% vs 9%). The efficacy and safety results obtained with Len/dex have led to this combination becoming a new standard of care for newly diagnosed MM patients, at least in the United States, and also a new backbone for combination with proteasome inhibitors and other novel agents.
Carfilzomib has been combined with Len/dex (CRd) in a pilot phase 1/2 trial in newly diagnosed MM patients, including young and elderly patients.25 Results of a subanalysis of 23 elderly MM patients showed impressive efficacy (100% ORR, with 65% stringent CR) and an acceptable toxicity profile (13% grade 1-2 PN). All patients remained free of progression and alive at the median follow-up of 1 year (Table 1). These results support a phase 3 study of CRd versus Rd in all age groups. Len/dex alone is also being compared with Len/dex plus Ixazomib (MLN9708) in a randomized trial in non-transplantation-eligible MM patients, supported by positive preliminary results with ixazomib in weekly schedule plus Len/dex (96% patients achieved at least PR, including 44% ≥VGPR and 26% CR) with good tolerability (Table 1).
Elotuzumab, an anti-CS1 monoclonal antibody, has proved to be safe and effective in combination with Len/dex in relapsed and refractory MM patients, and a randomized trial comparing Len/dex with or witout elotuzumab in newly diagnosed elderly MM patients is currently under way.
Is there any evidence that elderly patients need alkylating agents?
The Spanish group compared VMP with VTP in a randomized trial (see above) to identify the best partner for bortezomib, an alkylating agent or an immunomodulatory drug. VTP resulted in slightly greater efficacy (CR rate of 28% for VTP vs 20% for VMP), but also toxicity, especially cardiac side effects (11% with VTP and none with VMP) and PN (9% of grade 3-4 for VTP and 7% for VMP). The phase 3b UPFRONT trial evaluated the efficacy and safety of 3 bortezomib-based induction regimens, 2 non-alkylating-agent–based combinations, bortezomib with dexamethasone (VD) and bortezomib with thalidomide and dexamethasone (VTD), and one containing melphalan (VMP). The rate of PR or better was slightly higher for VTD (80% vs 73% for VD and 69% for VMP),26 but as in the Spanish trial, was also associated with a higher frequency of side effects, especially PN (24% of grade 3 or higher vs 19% for VD and VMP). No significant differences have so far been reported in terms of time-to-event data in both trials. Simultaneously considering efficacy, toxic effects, and costs, we concluded that melphalan is probably preferable to thalidomide for bortezomib-based combination therapy in the setting of elderly MM patients. Nevertheless, this conclusion cannot be extrapolated to lenalidomide, which has a better safety profile and greater efficacy than thalidomide.
The FIRST trial (IFM 07-01, MM-020) is currently comparing Len/dex until disease progression versus Len/dex up to 18 cycles versus MPT up to 12 cycles, with PFS as the primary end point. This trial will answer important questions about the treatment of newly diagnosed elderly MM patients, such as whether an alkylating-based combination is required or if Len-dex alone is sufficient and whether it is necessary to maintain treatment until disease progression or is it enough to provide it over a shorter period.
How can we improve and sustain the efficacy of treatment?
Despite the improvement in treatment responses and survival associated with the introduction of novel antimyeloma treatments, all patients with MM eventually relapse due to the persistence of residual disease. Recent data indicate that consolidation or long-term treatment can sustain remission by keeping the tumor under control. In elderly patients, the efficacy of long-term treatment should be balanced with tolerability and convenience of use.
Thalidomide maintenance
Three studies compared thalidomide maintenance after MPT (MPT-T) versus MP with no maintenance.9,10,27 All of these studies reported an improvement in TTP and PFS (or event-free survival), but only the Dutch-Belgian study9 found a significant improvement in OS for MPT-T compared with MP alone (40 vs 31 months, P = .05). However, the incidence of PN of grade 2 or above during maintenance was very high (54%). The MRC Myeloma IX trial of attenuated CTD versus MP also involved thalidomide maintenance randomization.28 Thalidomide maintenance therapy was associated with an improvement in PFS (P = .01), but OS was not significantly prolonged. Thalidomide maintenance was not well tolerated and patients remained on treatment for a median of only 7 months. Considered together, these studies indicate that thalidomide maintenance is not an attractive option in elderly patients due to its poor tolerability.
Bortezomib maintenance
The aforementioned Spanish study comparing VMP and VTP as induction therapies included a maintenance phase with either VT or VP for up to 3 years. Maintenance therapy improved the overall CR rate from 24% to 42%, with slightly higher values for VT than for VP (46% vs 39%; P = NS). PFS was 39 months in the VT group compared with 32 months in the VP arm (P = NS), with a trend toward better OS for VT (69% vs 50% at 5 years).29 Both regimens were well tolerated with no serious hematological toxicities, although VT maintenance was associated with a higher incidence of PN (9% vs 3%). The previously mentioned Italian trial that compared VMPT as an induction therapy with VMP also included a maintenance phase with VT in the former arm. Complete response rates after maintenance were increased to 38% in the VMPT-VT group. The median PFS was significantly longer with VMPT-VT than with VMP (37 vs 27 months; HR = 0.58; P < .0001), resulting in a significant benefit to OS (61% vs 51% at 5 years; HR = 0.70; P = .01).30 Maintenance with VT was well tolerated: grade 3 or 4 hematological AEs were reported by 3% of patients and grade 3 or 4 PN were found in 5% of patients. There are several studies currently under way that are investigating different bortezomib-based combinations with the aim of consolidating its role as a long-term treatment.
Lenalidomide maintenance
The efficacy and safety of continuous treatment with lenalidomide in elderly transplantation-ineligible patients has been evaluated in the MM-015 phase 3 study.14 After induction with MPR, in one arm, patients received maintenance with lenalidomide until disease progression (MPR-R), whereas the other MPR arm received no maintenance. PFS was significantly improved in the MPR-R group compared with MPR (31.0 vs 13.2 months, P < .001), with no differences so far in OS. Lenalidomide maintenance was as well tolerated as placebo, with very low rates of grade 3 or 4 thrombocytopenia, neutropenia, VTE, and fatigue (1%-3%). The 3-year risk of second primary tumors was 7%, confined to acute leukemias or myelodysplastic syndromes, and the interaction between melphalan and lenalidomide could increase the leukemogenic risk. However, the benefit of treatment appears to outweigh this risk of second primary tumors. When these efficacy and safety analyses were conducted in patients between 65 and 75 years of age, the benefit of continuous treatment with lenalidomide was more evident and thus could represent a new standard of care for this patient population. Although the concern about second primary tumors has decreased with longer follow-up, close monitoring is still needed. Several trials are currently under way that are also evaluating the role of lenalidomide in this patient population as a maintenance therapy, as a single agent, or in combination with prednisone or dexamethasone.
Finally, second-generation proteasome inhibitors are being evaluated as part of consolidation (carfilzomib in a modified schedule) or maintenance therapy (ixazomib weekly until disease progression).
Impact of novel drugs on the adverse prognosis associated with high-risk cytogenetics in elderly patients
Approximately 25% of elderly MM patients have cytogenetic abnormalities that are associated with a high risk of disease progression and very poor prognosis. High-risk cytogenetic profiles include del(17p), t(4;14), and/or t (14;16).31
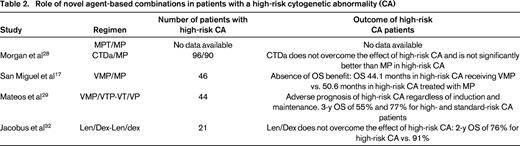
Table 2 summarizes the role of novel agents in the treatment of elderly MM patients with high-risk cytogenetic abnormalities. Data about thalidomide in patients with high-risk cytogenetic abnormalities are scarce. Recently, results from the Myeloma IX trial of CTDa as induction followed by thalidomide maintenance showed that PFS was not improved in patients with high-risk cytogenetics and OS was significantly shorter in the high-risk subset (P = .009).20
In the trial in which Len-Dex was compared with Len-dex, patients with high-risk cytogenetic abnormalities were less likely to attain VGPR (46% for standard-risk and 30% for high-risk patients). Moreover, high-risk patients showed shorter 2-year OS (91% for standard-risk and 76% for high-risk patients).32
In the VISTA trial of VMP versus MP, patients with high-risk cytogenetic profiles including the presence of a t(4;14),t,14,16 and/or a del(17p) had the same CR rate and similar TTP and OS times as patients with standard-risk cytogenetics, suggesting that the addition of bortezomib to MP was able to overcome the poor prognosis of these patients.15 However, due to the low patient numbers in this subanalysis (26 patients), caution is advised in interpreting these results. Moreover, updated information indicated that the final outcome of these patients was poorer than that of standard-risk patients.33 In the Italian study, the PFS benefit in response to VMPT plus VT maintenance over VMP was seen in patients with adverse cytogenetics and in standard-risk patients.19 In the Spanish trial, induction with VMP/VTP and maintenance with VP/VT were associated with similar response rates in patients with adverse compared with standard cytogenetics; however, these bortezomib-based regimens were unable to overcome the negative impact of high-risk cytogenetics, because the PFS and OS were significantly shorter in patients with t(4;14) and/or del(17p).34
The IFM group recently reported similar results in a series of 1890 elderly patients. The presence of t(4;14) and del(17p) was associated with shorter PFS and OS regardless of the treatment received, and this result was similar for patients younger or older than 75 years. In summary, the first generation of novel agents do not overcome the negative prognosis of high-risk cytogenetic abnormalities in newly diagnosed elderly patients with MM (Table 2).31
How to choose the best therapy option: individualized treatment strategies
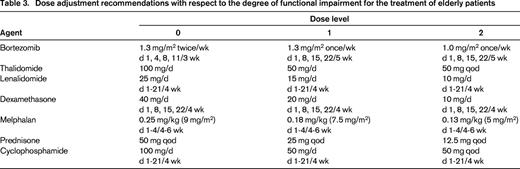
The various novel treatment combinations (Table 1), with or without alkylating agents, offer physicians the possibility of tailoring treatment approaches by taking an individual patient's profile and preferences into account. The first important consideration about this elderly population is that they are a heterogeneous group and many of them, regardless of their biological age, are physically frail, with multiple comorbid conditions (eg, diabetes, renal impairment, cardiovascular disease) and physical disabilities (eg, arthritis, dementia). In addition, tolerability is a key issue for them. A retrospective analysis of 1435 elderly patients receiving bortezomib and/or thalidomide in an up-front setting showed that the presence of features such as age ≥ 75 years or renal failure at presentation, occurrence of infections, cardiac or gastrointestinal AEs negatively affected survival.35 Therefore, all physicians treating elderly MM patients should undertake 3 actions before prescribing treatment: (1) assess the patient's biological age, comorbidities, frailty, and disability (it would be desirable to have simple geriatric surveys to evaluate whether a patient is frail); (2) evaluate the degree of functional impairment to select the most appropriate drug regimen, adapting the dose if required (Table 3)36 ; and (3) optimize the supportive care treatment with bisphosphonates, antibiotics, antivirals, anticoagulants, growth factors, and pain control.
Outside of clinical trials, the availability of novel drugs differs slightly from country to country and this clearly affects the choice of therapy. Bortezomib is used by most physicians around the world to treat elderly patients, but whereas most physicians outside of the United States offer MP-based combinations, in the United States, cyclophosphamide as an alkylating agent in combination with bortezomib or just bortezomib plus corticosteroid are the most commonly used. Of the immunomodulatory drugs, thalidomide is the most commonly used outside of the United States, in combination with MP or cyclophosphamide, whereas practice in the United States prefers lenalidomide to thalidomide.
For fit elderly patients without comorbidities or disabilities, one option would be an alkylating-containing triplet regimen such as VMP or MPT for up to 9 cycles or to complete 1 year of treatment. Their efficacy is proven and they have been approved for use. Their use has been optimized through the weekly and subcutaneous administration of bortezomib and by giving thalidomide at doses not higher than 100-200 mg. Another option would be to use a non-alkylator-based combination. Bortezomib plus dexamethasone is an available option that has been tested in the UPFRONT trial. In contrast, thalidomide plus dexamethasone is not well tolerated by elderly patients (at least at high doses). Len/dex, probably as continuous therapy until disease progression, is a very attractive option, but unfortunately has not yet been approved in most countries. Nevertheless, it is commonly used in the United States. VTD has also been tested in the Spanish and UPFRONT trials and, considering its efficacy and toxicity, should be restricted to fit patients without any (especially cardiac) comorbidities.
Another alternative approach would be to choose a sequential approach for fit patients (probably between 65 and 70 years of age): a non-alkylating-based induction regimen based on bortezomib and/or immunomodulatory drugs, followed by consolidation with alkylator-based approaches. Although conflicting results with Mel100-ASCT have been reported in the past, this possibility has reemerged for elderly patients after the arrival of novel agents. It has been explored in a phase 2 trial administering bortezomib, pegylated liposomal doxorubicin, and dexamethasone (PAD), followed by tandem melphalan 100 mg/m2 with stem cell support and consolidation with Len/dex and maintenance with lenalidomide alone.19 The CR rate after Len/dex and Len consolidation/maintenance was 53%, with a median PFS of 48 months and 83% of patients alive at 5 years. These promising results support this option for selected fit patients between the ages of 65 and 70 years. However, the use of consolidation and maintenance with Len/dex are not approved and should currently be restricted to clinical trials.
For unfit elderly patients, dose adjustments are key to improving tolerability. Bortezomib should always be given in a weekly scheme and as a subcutaneous formulation, probably in combination with low-dose steroids (prednisone may be better tolerated than dexamethasone), considering a low dose of melphalan or, as a probably better alternative, cyclophosphamide. Oral drugs can be more convenient for frail elderly patients; lenalidomide can be given at a standard dose with low-dose dexamethasone, whereas thalidomide should not be given at doses higher than 50-100 mg daily in combination with oral cyclophosphamide and prednisone on alternate days. The toxicity and efficacy of the treatment should be evaluated every cycle to try to obtain the maximum benefit of this tailored approach of therapy and to avoid overtreatment and the development of unexpected toxicity.
Other factors should be considered when making treatment decisions. In patients who have a history of VTE, a bortezomib-based combination may be a preferred treatment choice because it is less thrombogenic. However, appropriate anticoagulant prophylaxis has been shown to reduce VTE complications to ∼3% in patients treated with lenalidomide- or thalidomide-containing regimens. In patients with preexisting neuropathy, MPR, Rd, or bendamustine plus prednisone would be a good choice for up-front treatment because these are not associated with neurotoxicity. In patients with renal failure, bortezomib, thalidomide, and bendamustine can be administered at the full approved dose; lenalidomide requires adjustments of the starting dose based on creatinine clearance.37
For maintenance therapy, our current information indicates that continuous long-term therapy prolongs the TTP; however, no OS benefit has been noted so far. Accordingly, maintenance approaches should be restricted to clinical trials to address unanswered questions such as whether maintenance should be given for all patients, whether there are any clinical or biological characteristics predicting benefit from continuous therapy, and which drug and dose are optimal, and to define optimal duration of treatment.
With respect to the presence of high-risk features, there is not yet enough evidence to make specific recommendations, although some studies indicate that proteasome inhibitors may be of some value in these patients.
Conclusions and future perspectives
The availability of new combination regimens, including the novel agents thalidomide, bortezomib, and lenalidomide, has improved the treatment options for elderly patients with MM. The combination of MPT, VMP MPR, and Len-dex provides a new standard of induction for elderly patients. Other combinations, including the second and third generation of novel drugs, are also under clinical development. Maintenance treatment with novel agents is emerging as a new strategy to sustain disease control and delay disease progression; however, longer follow-up is needed to assess the optimal duration and final benefit to OS. The optimal treatment approach should provide a good balance of efficacy and safety against costs. Moreover, quality of life should also be evaluated, because this is not captured by the response criteria. All of these novel agent-based combinations are resulting in deeper and longer remissions, but we also need optimized tools to monitor our patients (minimal residual disease assessments, novel imaging techniques, etc) in parallel with the development of new drugs.
Disclosures
Conflict-of-interest disclosure: M.-V.M. has received honoraria from Janssen, Celgene, Onyx, Millennium, and Mundipharma. J.F.S.M. is on the Board of Directors or an advisory committee for Janssen, Millennium, Celgene, Novartis, and Onyx. Off-label drug use: lenalidomide is not approved for its use as first line of therapy; carfilzomib is not approved for its use as first line of therapy.
Correspondence
María-Victoria Mateos, Hospital Universitario de Salamanca, Paseo San Vicente 58-182, 37007 Salamanca, Spain; Phone: 034-678-438203; Fax: 034-923-294624; e-mail: mvmateos@usal.es.