
Abstract
Although the median age for adults with acute lymphoblastic leukemia (ALL) is older than 60 years, relatively few of these patients have been enrolled on prospective clinical trials. The presence of coexisting medical disorders and unfavorable cytogenetic and biological characteristics within this population presents considerable challenges for successful treatment using conventional chemotherapy programs. Selected patients have achieved remission and long-term survival following intensive chemotherapy. Preliminary data using several new agents that have shown promise for patients with ALL are described.
The success that has been achieved in treating children and younger adults with acute lymphoblastic leukemia (ALL) has not been paralleled in older adults. Likely reasons include the presence of coexisting medical disorders leading to decreased tolerance for chemotherapy as well as fundamental biological differences in the spectrum of ALL seen in this population. In this review, as in most of the available literature, the older adult age group is generally 60 years and older, although some series start at 55 years and others at 65 years old.
Age-related Clinical and Biological Differences
Available data on ALL in older patients are relatively scarce. One population-based registry reported that 31% of all cases occurred in patients 60 years or older. Although the most common malignant disease in childhood, ALL is rare in adults.1 The age-specific annual incidence in the United States is only 0.4 to 0.6 cases per 100,000 individuals between 25 and 50 years old (Figure 1 ). However, the incidence rises steadily during the older decades and is two- to threefold higher above the age of 60 years (0.9 to 1.6 cases per 100,000). According to the US Census Bureau, one-fifth of the population in 2050 will be older than 65 years; the fastest growing segment of the elderly population is 85 years and older.
There is considerable evidence that the clinical and biological characteristics of the disease change dramatically between childhood, the middle adult years, and older age groups. For example, the ratio of males to females declines from 1.75 in younger adults to 0.97 in older adults. Comparative data on clinical characteristics are available from large treatment centers, although these are not free of referral bias. Sixty-nine patients between 60 and 89 years old (median, 68) were evaluated at the Hopital Edouard Herriot in Lyon, France, between 1980 and 1998, and were compared with 309 younger adults 15–59 years old (median, 29).2 Of note, 14% of the older adults had previously had a malignant disease compared with 3% of the younger patients. The older adults were less likely to have peripheral lymphadenopathy (21% vs 51%) or a mediastinal mass (1% vs 14%) or splenomegaly (26% vs 45%), but there were no differences in hepatomegaly or central nervous system involvement. Weight loss was slightly more common among older patients, but fever, infection and bleeding were less common.
Modest differences were noted in presenting blood counts. The median white blood cell (WBC) count was 8400/μL (range, 500–520,000/μL) among the older patients compared with 13,200/μL (range, 500–1,440,000/μL) among the younger adults (P = 0.05). There were no differences in the initial median hemoglobin levels (9.7 g/dL vs 10.1 g/dL) or platelet counts (47,000/μL vs 55,000/μL).
The most significant differences were noted in the immunophenotypic and karyotypic results. Lymphoblasts were of B-cell lineage in 89% of the older patients compared with 66% of the younger adults (P = 0.0004). Conversely, T-cell ALL was present in only 8% of older patients but 29% of the younger patients (P = 0.0007). Myeloid antigens were co-expressed by 19% of the older adult cases compared with 11% of the younger cases; lymphoblasts from 69% of older ALL patients also expressed CD34. A similar analysis has been reported by the German Multicenter ALL Study Group (GMALL), although the older age group was truncated at 65 years old.3 Between 1984 and 1999, 342 patients (12%) 55–65 years old were enrolled on one of four prospective clinical trials and were compared with 2463 patients (88%) ages 15–54 years. The older patients less frequently had peripheral lymph node involvement, mediastinal tumor, or splenomegaly. The frequency of a common or pre-B immunophenotype was higher among older patients (75% vs 59%; P = 0.001) whereas T-cell ALL was less frequent (3% vs 14%) and the frequencies of null plus pro-B ALL were similar (13% vs 12%). Among T-ALL cases, mature T-ALL (2% vs 7%) and thymic T-ALL (3% vs 14%) occurred less commonly in older patients. In a recent multicenter series of older ALL patients from Poland, no remarkable differences in pretreatment characteristics were reported between 64 patients 60–69 years old and 23 patients 70 years and older.4
Age-Related Cytogenetic Differences
Cytogenetic abnormalities characterize the biological heterogeneity of ALL and provide a strong and independent prognostic factor for treatment outcome.5 The incidence of Philadelphia (Ph) chromosome–positive ALL, a subset that is resistant to conventional chemotherapy, clearly increases with age.6 Clonal chromosomal abnormalities were found at diagnosis in 378 of 443 adults (85%) by the Groupe Francais de Cytogenetique Hematologique; 60 (13%) were older than 60 years (range, 60–84).7 In this series, 18% of those less than 40 years old and 46% of those 40–60 years old were Ph+ compared with 35% of those older than 60 years. Among 276 patients (ages 16–83) with centrally reviewed karyotypes enrolled on a prospective study by the Cancer and Leukemia Group B (CALGB), 76% had a clonal abnormality; 28% overall and 33% of those older than 60 years had a t(9;22).8 In a recent report from the Southwest Oncology Group, the frequency of Ph+ ALL increased from 6% in those less than 25 years old to 14% for those 25–35 years old, 33% for those 36–55 years old, and 53% for patients older than 56 years.9 In the large GMALL series described above, among those with common or pre-B ALL, the incidence of Ph+ or BCR/ABL+ ALL was significantly higher among adults older than 55 years than younger adults (54% vs 37%; P = 0.001).3 In the French series from Lyon, the Ph chromosome or BCR/ABL fusion gene was detected in 24% of older patients and 19% of young patients.2 In contrast, a rearrangement of chromosome 11q23 was observed in only 2% of older and 5% of younger patients (χ2 statistic, P = 0.001). An analysis of the age distribution of chromosomal abnormalities in 1500 British cases of ALL has been reported.10
Prospective Clinical Trials in Older Adults
With a few exceptions, older patients with ALL have often been excluded from clinical trials by eligibility criteria. Regimens developed for younger adults have been truncated at 60 or 65 years old. For the past two decades, the CALGB has not had an upper age limit for enrollment onto its frontline ALL treatment studies. Approximately 18% of clinical trial subjects have been 60 years or older (median, 66 years; range 60–83 years). Similarly, investigators at the M.D. Anderson Cancer Center in Houston, Texas have actively enrolled older patients in their frontline ALL studies.11 The fraction older than 60 years has been 22%. In both this multicenter example and a single center experience, the proportion of older patients enrolled appears less than the prevalence of ALL in the community.
In general, older cancer patients have been under-represented in prospective clinical trials, and this can have serious consequences on the development of better therapies for these patients.12 This is particularly notable for patients greater than 75 years old. Although it is estimated that 54% of patients with leukemia in the United States are greater than 65 years old, only 24% of subjects enrolled on new drug trials for leukemia filed with the US Food and Drug Administration (FDA) are older than 65 years.13 In the United Kingdom, where on average 68 patients 60 years or older develop ALL every year, only 3–8 patients (4%–15%) were enrolled each year on the national MRC UKALL X and XA studies.14 Criteria for decision-making regarding which older patients should be recommended for treatment have not been adequately addressed.
Very few clinical trials have focused on therapies designed specifically for older patients with ALL, and fewer still have sufficient numbers to deal with the clinical and biological heterogeneity within this age group. Even when treated on the same trial as younger adults, older patients often receive attenuated doses of myelosuppressive drugs.15,16Figure 2 demonstrates the effect of increasing age on the outcomes of 759 adults with newly diagnosed ALL treated on 5 sequential CALGB studies between 1988 and 2002. The complete remission (CR) rate declined from 90% for those under age 30, to 81% between 30–59 years old, and to 57% for those 60 years and older. The overall survival at 3 years was estimated to be 58% (95% confidence limits, 52%–64%) for those less than 30 years old, 38% (33%–43%) for those 30–59 years old, and only 12% (7%–19%) for the 129 patients older than 60 years. Similar results have been reported by other cooperative groups and large leukemia centers (Table 1 ).
The GMALL Study Group reported on a pilot study designed for patients older than 65 years.17 Favorable factors for achievement of CR were Pro-B ALL or T-ALL (69% compared with 36% for pre-B ALL), no Ph chromosome (64% vs 19% for Ph+), and WBC count < 30,000/μL (60% compared to 25%). The CR rate was 74% for patients without any of these risk factors. In contrast, 52% of patients had one or more of these risk factors, and they had a CR rate of only 19% (P = 0.001). Survival was also significantly better for the group with no risk factors (median, 17 months compared to 6 months, P = 0.002). Recently updated to include 94 patients, the CR rate overall was 48% but survival was less than 10%.18 Both Hoelzer and Pagano et al have recently reviewed the literature describing the outcomes of older ALL patients reported between 1990 and 2004.19,20 Taken altogether, the weighted mean CR rate was 56% for the 519 patients older than 60 years who received intensive chemotherapy on a prospective trial; 23% of patients had early deaths, and 30% had chemotherapy-resistant disease. The median remission duration was 9 months, and the median survival overall was 7 months.
Palliative chemotherapy approaches are sometimes recommended to older patients because of poor performance status or the presence of co-morbid disorders such as diabetes, cardiac disease, or renal insufficiency. In a report from the Instituto di Demeitotica Medica in Rome, 37 (31%) of 119 patients, newly diagnosed with ALL between 1986 and 1998, were older than 65 years; 25 received intensive chemotherapy and 12 received only vincristine and steroids.21 A CR was achieved in 80% of the intensively treated older patients and their median survival was 14 months (range, 2–82). Among the patients managed with palliative treatment, 42% had a CR; the median survival for all 12 patients was only 2.6 months (range, 0.3–19).
Similar results were reported when practice patterns in the Northern Region of England were surveyed.22 Among 62 consecutive, newly diagnosed ALL patients older than 60 years, 28 (median age, 67 years; range, 60–80) received “curative” therapy, 25 (median age, 74) received palliative therapy, and 9 (median age, 83) received no treatment. A CR was achieved in 10 (36%) of the intensively treated group and 4 (16%) of the palliative therapy group. The median survival for each treatment group was only 3 months, although several patients survived longer than 3 years after intensive therapy.
Management of Older Patients with ALL
Pharmacologic changes associated with aging do not necessarily apply to all persons above a specific age.23,24 Co-morbid conditions, interactions with multiple other medications, nutritional status, and adherence to complex treatment regimens all influence the pharmacokinetic profile in older adults. There is little evidence that drug absorption is affected by the chronological age of the patient. However, the volume of distribution of a drug may be less than in younger adults due to different proportions of body fat to lean body mass, hydration status, and plasma protein levels. Hepatic blood flow and renal clearance may be diminished in older patients. However, older adults with normal calculated renal function appear to tolerate chemotherapy drugs and have similar toxicity profiles as younger adults.
Nevertheless, the pharmacodynamic effects of particular drugs may be greater in older individuals. The number of hematopoietic stem cells declines with age; thus, the neutrophil nadir may be lower and recovery from myelotoxic chemotherapy more prolonged in older adults.25 Mucositis appears to be more frequent and more severe in older patients, and the consequences with regard to pain, diminished nutrition, and infection may be more grave. Pain may respond to considerably lower doses of analgesics in older patients. Delirium during treatment is under-recognized and misdiagnosed. It must be treated promptly by removing the causative factors or with psychotropic medications such as haloperidol. Interestingly, nausea and vomiting after chemotherapy have been reported to be less common in older adults.
Specific leukemia drugs have well known toxicities that require special attention in older patients. Vincristine may cause severe constipation, and laxatives should be used prophylactically. Corticosteroids can exacerbate diabetes, and hyperglycemia may lead to infection and fluid and electrolyte abnormalities. l-asparaginase causes cognitive impairment leading to encephalopathy more often in older adults than in children. The appearance of somnolence and confusion in such cases can be mistakenly attributed to depression or viral encephalitis. Discontinuation of the enzyme and prompt refeeding or infusion of amino acid solutions containing glutamine can yield a dramatic improvement in mental status. Discontinuation of extraneous medications that many older adults take for chronic but mild disorders can prevent serious drug interactions during chemotherapy.
Among randomized clinical trials testing the use of hematopoietic growth factors during chemotherapy for ALL, older patients have enjoyed the greatest benefits. In a CALGB study of 185 ALL patients who were randomly assigned to receive either granulocyte colony-stimulating factor (G-CSF) or a placebo during induction and consolidation therapy, 36 were 60 years or older.15 The time to recovery of > 1000 neutrophils/μL during remission induction was shortened from 29 days in the placebo group to 16 days in the G-CSF group (P < 0.001). For these older patients the corresponding CR rates were 69% in the placebo group and 85% in the G-CSF group, and the induction death rate fell from 31% to 5% with G-CSF support. Older patients who received placebo had a median time to platelet recovery > 50,000/μL of 26 days, whereas the older patients who received G-CSF had a median of 17 days. It has become routine practice within the CALGB to use G-CSF during treatment of ALL in older adults.
Newer Drugs for ALL
It is not likely that escalating the doses of currently available chemotherapy agents or altering their sequence of administration will markedly improve the outcome of treatment for ALL in adults. New drugs are needed. Because a large fraction of older patients have Ph+ ALL, major advances in the treatment of BCR/ABL+ leukemia offer hope for considerable improvement. Ottmann and Wassmann (see “Treatment of Philadelphia chromosome–positive acute lymphoblastic leukemia” in this volume) have detailed the evidence that the tyrosine kinase inhibitor imatinib mesylate should be incorporated into induction and post-remission therapy for these patients. Second generation ABL kinase inhibitors such as AMN107 (Novartis) and dasatinib (BMS354825; Bristol-Myers Squibb) are now completing phase II trials in patients with imatinib-resistant Ph+ ALL. If successful, these agents should be evaluated next in front-line therapy and in combination with chemotherapy.
Other targeted therapies currently being evaluated in ALL include monoclonal antibodies. Rituximab binds to CD20, which is expressed on more than 20% of lymphoblasts in about half of common or pre-B ALL cases. Investigators at the MD Anderson have incorporated rituximab into frontline hyper-CVAD therapy for CD20+ ALL.26 In a pilot study by the GMALL, when rituximab was given before each cycle of chemotherapy, the CR rate was 63% and survival after one year was 54% for 19 CD20+ patients older than 55 years (median, 66).18
The antigen CD52 is expressed on normal and malignant lymphocytes and is the target for alemtuzumab. Approved for the treatment of B-cell chronic lymphocytic leukemia, this antibody has also shown single-agent activity in a small number of patients with refractory ALL. It is currently being tested in both young and older adults with CD52+ ALL in first remission by the CALGB. Approximately 69% of ALL cases have been shown to express CD52 on >10% of the blasts. A dose-escalation pilot study has demonstrated the safety of administering 30 mg subcutaneously 3 times per week for 4 weeks between courses of intensive consolidation chemotherapy at a time when minimal residual disease is likely to be present.
The newest drug to be approved by the FDA for the treatment of ALL in children is clofarabine.27 This purine analog has also shown single-agent activity in adults with relapsed ALL or acute myeloid leukemia (AML) and has been combined with cytarabine for initial treatment of older patients with AML or myelodysplastic syndrome. Clof-arabine acts by inhibiting ribonucleotide reductase and DNA polymerase, depleting the amount of intracellular dNTPs available for DNA replication and also resulting in premature DNA chain termination. Dose limiting toxicities have been reversible hepatotoxicity and rash.
Nelarabine (compound 506U78; GlaxoSmithKline) has completed phase II trials in both children and adults with relapsed or refractory T-ALL.28 Although neurotoxicity has been dose-limiting, the drug can be given safely at 900 mg/m2/day by continuous intravenous infusion for 5 days in children, or at 1.5 g/m2/day on days 1, 3 and 5 in adults.29,30 Nelarabine has considerably less activity against B-lineage ALL. Forodesine (BioCryst; BCX-1777), a novel inhibitor of purine nucleotide phosphorylase, has shown activity in cutaneous T-cell lymphoma and is now being investigated in phase I and II trials in relapsed T-ALL.31 However, because of the low incidence of T-ALL in patients older than 60 years, these latter two drugs are unlikely to impact on the outcomes of many older patients.
Drugs with proven efficacy against ALL, such as vinc-ristine and daunorubicin, have been modified as liposomal sphingomyelin/cholesterol preparations, and are in clinical trials.32 The liposomal preparations offer the ability to infuse higher total doses of the native drug, yielding greater tumor cell uptake with no increase in neurotoxicity or cardiac toxicity.33 Liposomal encapsulation provides pharmacokinetic advantages such as a prolonged half-life compared with the free drug and possibly preferential uptake into tumor cells. Italian investigators have reported on a small trial using liposomal daunorubicin with vincristine and dexamethasone in 15 newly diagnosed older ALL patients (median age, 69 years).34 The CR rate was 73%, the median disease-free survival (DFS) was 21 months, and the 2-year DFS was 36%.
Many new drugs await further testing and incorporation into frontline regimens (Table 2 ).35 It is possible that some combination of these agents will overcome the innate resistance present in older patients with ALL and at the same time improve the overall tolerance to treatment.
Treatment outcomes for young, middle-aged, and older adults with acute lymphoblastic leukemia (ALL).
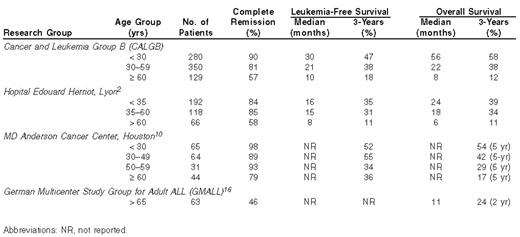
Abbreviations: NR, not reported.
New drugs under development for acute lymphoblastic leukemia (ALL).
| New Agent | Mechanism | Notes |
|---|---|---|
| Monoclonal Antibodies: | ||
| Rituximab | Anti-CD20 | May potentiate chemotherapy in B-cell malignancies |
| Alemtuzumab | Anti-CD52 | Can be given IV or subcutaneously |
| Antimetabolites: | ||
| Clofarabine | Nucleoside analog; inhibits ribonucleotide reductase and DNA polymerase | Approved for relapsed childhood ALL |
| Nelarabine | Pro-drug of ara-G. | Effective in T-ALL |
| Inhibits purine nucleoside phosphorylase (PNP). | ||
| Forodesine | Inhibits PNP | Under evaluation in T-ALL |
| Trimetrexate | Competitive inhibitor of dihydrofolate reductase | Not dependent upon facilitated transport into cells |
| Aminopterin | Anti-folate | Excellent oral bioavailability |
| Liposomal encapsulated drugs: | ||
| Liposomal vincristine | Diminished neurotoxicity | |
| Liposomal daunorubicin | Diminished cardiotoxicity | |
| Pegylated asparaginase | Long half-life (6 days) | |
| New Agent | Mechanism | Notes |
|---|---|---|
| Monoclonal Antibodies: | ||
| Rituximab | Anti-CD20 | May potentiate chemotherapy in B-cell malignancies |
| Alemtuzumab | Anti-CD52 | Can be given IV or subcutaneously |
| Antimetabolites: | ||
| Clofarabine | Nucleoside analog; inhibits ribonucleotide reductase and DNA polymerase | Approved for relapsed childhood ALL |
| Nelarabine | Pro-drug of ara-G. | Effective in T-ALL |
| Inhibits purine nucleoside phosphorylase (PNP). | ||
| Forodesine | Inhibits PNP | Under evaluation in T-ALL |
| Trimetrexate | Competitive inhibitor of dihydrofolate reductase | Not dependent upon facilitated transport into cells |
| Aminopterin | Anti-folate | Excellent oral bioavailability |
| Liposomal encapsulated drugs: | ||
| Liposomal vincristine | Diminished neurotoxicity | |
| Liposomal daunorubicin | Diminished cardiotoxicity | |
| Pegylated asparaginase | Long half-life (6 days) | |

Age-specific annual incidence of acute lymphoblastic leukemia (US-SEER data, 1998–2002).
Age-specific annual incidence of acute lymphoblastic leukemia (US-SEER data, 1998–2002).

Treatment outcome by age cohort (CALGB studies with 759 acute lymphoblastic leukemia (ALL) patients, 1988–2002).
Treatment outcome by age cohort (CALGB studies with 759 acute lymphoblastic leukemia (ALL) patients, 1988–2002).
Department of Medicine and the Cancer Research Center, University of Chicago, Chicago IL
