
Abstract
Newly diagnosed aplastic anemia is a serious condition, with more than 75% (higher in young patients) becoming long-term survivors if diagnosed and treated appropriately. First-line treatment approaches include immunosuppressive treatment using the combination of antithymocyte globulin and cyclosporine A for patients without a sibling donor and HLA identical sibling transplant for patients younger than age 40 with a donor. Best transplant strategies have been defined and include conditioning with cyclophosphamide and antithymocyte globulin, marrow as a stem cell source, and graft-versus-host diease prophylaxis using cyclosporine A and methotrexate. It is against these standard treatment approaches that any therapeutic progress has to be measured.
Aplastic anemia (AA) is defined as pancytopenia with a hypocellular marrow. The incidence of acquired AA in the Western hemisphere is around 2 per million population per year and higher in East Asia. Age distribution shows peaks in children and young adults and again in patients age > 60 years. AA is, in most cases, an acquired autoimmune disorder; congenital AA is not the topic of this review. Patients with AA commonly present with anemia and hemorrhage and, more rarely, neutropenic infection. Severe AA (SAA) is defined by at least two of the following: reticulocytes < 50 × 109/L (or 20 × 109/L by manual counting), platelet count < 20 × 109/L, and neutrophil count < 0.5 × 109/L. In very severe SAA (vSAA) neutrophil counts are < 0.2 × 109/L. Often, the diagnosis is not very clear at the outset. Marrow cellularity is not always easy to assess and varies with age (ie, a normocellular marrow in an octagenerian is considered hypocellular in a child). In healthy older patients, subcortical marrow tends to be acellular. In general hypocellularity by biopsy is more reliable than by cytology. Patients may require more than one biopsy to confirm the diagnosis. Treatment decisions are complex; a watch and wait strategy is often used initially in a case of unexplained pancytopenia, but an interval from diagnosis to treatment of more than 1 to 2 months may be associated with worse outcome.1 Prior to treatment, the patient should be stable in terms of controlling bleeding and treating infection. Spontaneous recovery is rare. Once the patient is clinically stable, the disease is confirmed, disease severity is assessed, and family typing done. It is usually time to initiate treatment rapidly.
First-line Treatment
Decision for first-line treatment will depend on patient age, availability of an HLA identical sibling donor, and, in part, on the severity of the disease.2 Family typing is, therefore, recommended at first suspicion of the disease. The standard first-line treatment for a newly diagnosed patient with AA is either allogeneic bone marrow transplantation (BMT) from an HLA-identical sibling donor or immunosuppressive therapy (IST) with a combination of antithymocyte globulin (ATG) and cyclosporine A (CSA; ATG + CSA) (Figure 1).

HLA-Identical Sibling Donor Transplantation
Transplantation for AA from an HLA-identical sibling donor has improved considerably over the years, with a 75% to 80% chance of long-term cure (Figure 2). Unresolved issues are graft failure rates of 4% to 14% and graft-versus-host (GVHD), severe acute GVHD (grade III/IV)—which appears to occur less commonly now—and chronic GVHD that still occurs in 30% to 40% of patients.

HLA-identical sibling transplantation for AA as first-line strategy, data reported to the EBMT database 1975 to 2009. Ten-year survival is 34% ± 8% for patients transplanted 1975 to 1980 (n = 142); 60% ± 4% for patients transplanted 1980 to 1990 (n = 701), 73% ± 3% for patients transplanted 1990 to 2000 (n = 1377); and 79% ± 2% for patients transplanted 2000 to 2009 (n = 1951).
HLA-identical sibling transplantation for AA as first-line strategy, data reported to the EBMT database 1975 to 2009. Ten-year survival is 34% ± 8% for patients transplanted 1975 to 1980 (n = 142); 60% ± 4% for patients transplanted 1980 to 1990 (n = 701), 73% ± 3% for patients transplanted 1990 to 2000 (n = 1377); and 79% ± 2% for patients transplanted 2000 to 2009 (n = 1951).
Allogeneic BMT from an HLA-identical sibling donor is recommended as first-line treatment if the disease is severe or very severe, and if the patient is younger than age 40 years. There is controversy concerning the upper age limit for BMT as a first-line treatment because results vary in different case series. As shown in Figure 3, it has been the current practice in Europe to analyze outcome after BMT by age and to define an age cutoff with worse survival for older patients. It appears that this cutoff is undergoing a shift toward patients older than 50 years, as in more recent cohorts outcome of patients in the ranges of 20 to 30 years, 30 to 40 years, and 40 to 50 years tend to be similar. The advantage of treating a patient with IST and transplanting only in case of IST failure is appealing, but outcome in patients undergoing transplantation after failing IST is worse than undergoing transplantation upfront.3 In this study, the hazard ratio for mortality was 1.7, compared with patients with upfront transplantation. The recommendation within the recently completed European Group for Blood and Marrow Transplantation (EBMT) treatment algorithm is to use a cutoff of 40 years.

Impact of age on outcome after transplantation from an HLA-identical sibling 1999 to 2009. In 2316 patients reported to the EBMT database, irrespective of whether the transplant was the first or a subsequent treatment. Five-year survival probabilities are 85% ± 2%, 77% ± 4%, 71% ± 7%, 68% ± 8%, and 48% ± 10% in the age groups < 20, 21 to 30, 31 to 40, 41 to 50, and > 50 years.
Impact of age on outcome after transplantation from an HLA-identical sibling 1999 to 2009. In 2316 patients reported to the EBMT database, irrespective of whether the transplant was the first or a subsequent treatment. Five-year survival probabilities are 85% ± 2%, 77% ± 4%, 71% ± 7%, 68% ± 8%, and 48% ± 10% in the age groups < 20, 21 to 30, 31 to 40, 41 to 50, and > 50 years.
For patients with an HLA-identical sibling donor in whom transplantation is not used as first-line treatment, BMT remains an option as second-line treatment in the case of IST failure.
Optimal transplantation strategies for HLA-identical sibling BMT have been defined.
Stem Cell Source and Donor Selection
It is recommended bone marrow stem cells be used rather than granulocyte-colony stimulating factor (G-CSF) mobilized peripheral blood stem cells (PBSCs). In a retrospective combined Center for International Blood and Marrow Transplant Research (CIBMTR) and EBMT study, earlier engraftment occurred with PBSC without difference in graft rejection. Survival was worse with more chronic GVHD, using PBSC compared with bone marrow.4 Umbilical cord blood as an alternative source of stem cells for transplantation has been used in a small number of patients with AA. Outcome is excellent in the case of identical sibling cord (a situation that is rare; ie, child with the disease of a mother who is pregnant), but much less so with unrelated cord blood units. The effect of sex-mismatch between donor and recipient has been evaluated in a large retrospective EBMT. Survival was better in patients with donors from the same sex. Male patients with female donors had risks of acute GVHD increased by 33%, compared with male into male transplant patients; female patients with male donors had increased risks (220%) of graft rejection.5
Conditioning and GVHD Prophylaxis
The conditioning regimens and GVHD prophylaxis described below refer specifically to patients with acquired AA. In younger patients with AA, the standard conditioning proposed by the Working Party on SAA (WPSAA) is cyclophosphamide 50 mg/kg 32 × 4 + ATG. This regimen is nonmyeloablative and highly immunosuppressive to prevent graft rejection and GVHD. The benefit of adding ATG to cyclophosphamide is unclear, because a recently published prospective randomized clinical trial (RCT) from CIBMTR showed no significant benefit in terms of graft rejection, GVHD, and survival rates, compared with cyclophosphamide alone.6 Raw unadjusted data, from the EBMT database, show a slightly superior 10-year survival of 85% versus 75% when ATG is used as part of the conditioning regimen in sibling donor transplantation. The recommended posttransplant immunosuppression is CSA continued for at least 12 months, with slow tapering and short course methotrexate—the superiority of the combination having been confirmed in an RCT,7 but the optimal duration of immunosuppression with CSA posttransplant is not known. Because of unsatisfactory results with older patients (eg, age > 30 or > 40 years) with sibling donor transplantation, factoring in that most of these patients received a transplant not as first-line, but as second-line treatment having a longer interval from diagnosis to transplantation and a higher transfusional load; several groups have tried to modify conditioning by adding (eg, fludarabine) and by reducing the cyclophosphamide dose. Some interesting series have been published,8 although no prospective clinical trial has been run.
There is a significant risk of late graft failure in AA following allogeneic BMT possibly associated with discontinuing CSA early. Late graft failure may follow progressive mixed chimerism, defined by > 10% recipient cells or > 15% increase over 3 months; rarely is late graft failure hidden by autologous reconstitution.9,10 Stable mixed chimerism is associated with excellent survival and a low risk of chronic GVHD.
The EBMT WPSAA has recently activated an observational audit (http://www.ebmt.org), where treatment recommendations for first and subsequent lines of treatment are detailed for all age groups incorporating the lessons learned in the trials as detailed previously.
The EBMT activity survey shows that bone marrow transplant activity for marrow failure continues to increase in Europe, from approximately 200 transplants per year in the early 1990s to about 600 transplants per year in 2008. This increase is, to a large part, due to patients receiving transplants from unrelated donors, mostly after having failed immunosuppression.11
Immunosuppressive Treatment
ATG and CSA
IST, using the combination of ATG + CSA, is associated with response rates of 60% to 80%, with current 5-year survival rates of around 75%.12–16 Survival is better in younger than in older patients, as shown in Figure 4. Response definition includes a confirmation by two or more blood counts at least 4 weeks apart, in patients not receiving growth factors. Partial response is defined by transfusion independence, whereas normalization of blood counts is required for complete remission.17 Following ATG + CSA, patients should be followed for response, relapse, and late clonal disorders, such as paroxysmal nocturnal hemoglobinuria (PNH), myelodysplastic syndrome (MDS), and acute myeloid leukemia. There are no good predictors of response to IST, although a recent study by the National Institutes of Health (NIH) has shown that response at 6 months is associated with age, absolute reticulocyte count, and absolute lymphocyte count.18 In a recent EBMT study randomizing patients between concomitant treatment with G-CSF versus none, neutrophil response to G-CSF was associated with better survival in a post-hoc analysis.19 These factors are interpreted as reflecting disease severity moreso than the true autoimmune nature of the disease. Patients failing a first course of IST or relapsing after initial response may respond to a second course.20,21 A second course should not be initiated earlier than 4 to 6 months after the first course, because it usually takes more than 3 months before a response occurs. There is a 30% to 60% chance of response to a second course. There are patients refractory to two courses of IST who will not respond to a 3rd and who are considered true IST refractory cases.22 In these patients, the pathophysiology of the disease may be different, although there are no tools at this point in time to distinguish them from responding AA patients. Early identification of IST refractory cases is obviously needed, because these patients may be treated by other means (eg, alternative donor stem cell transplantation).

Survival at 10 years after immunosuppression as first-line treatment strategy in 3202 patients treated between 1975 and 2009 by decade (1970s, 1980s, 1990, and 2000s), and reported to the EBMT database.
Survival at 10 years after immunosuppression as first-line treatment strategy in 3202 patients treated between 1975 and 2009 by decade (1970s, 1980s, 1990, and 2000s), and reported to the EBMT database.
To analyze long-term outcome event-free survival is much more important than survival alone; events are defined as primary nonresponse, relapse, and secondary clonal complications, such as MDS/leukemia and PNH. Event-free survival after ATG + CSA is typically in the 35% to 50% range at 5 years.12 Response to ATG and CSA occurs late, typically 3 to 6 months after treatment. Response is stable in many patients, but relapse may occur. This is typically reported to be around 30% within the EBMT; reported rates vary among groups. Patients are at risk of late clonal complications; typically, rates are around 8% for MDS/acute myeloid leukemia, 10% for hemolytic PNH, and 11% for solid tumors at 11 years, as reported by the German SAA Study Group.
First-line treatment by IST is indicated for patients not eligible for sibling donor BMT. This includes patients with transfusion-dependent, nonsevere AA and patients with SAA or vSAA who are age > 40 years and younger patients with SAA or vSAA who lack an HLA-compatible sibling donor. For patients who are not transfusion- dependent, it may be reasonable to follow the patient without intervention.
ATG is a powerful immunosuppressive, and its use in severely neutropenic patients requires careful monitoring, prophylaxis, and treatment of infections, as well as adequate (and sometimes intensive) platelet transfusional support. In Europe, the standard preparation of ATG has until recently been horse ATG (Lymphoglobuline; Genzyme Corporation, Cambridge, MA) whereas in the United States, ATGAM Company (Upjohn, Kalamazoo, MI) has been used in a slightly different dosage. All large European Cooperative Studies have been done using horse ATG. The European preparation has been recently withdrawn from the market and replaced by a rabbit ATG (Thymoglobuline; Genzyme), up to now used for second or subsequent courses of IST21,23 (Table 1). Response rates to rabbit ATG are anticipated to be similar to horse ATG, based on response rates to second courses of IST, the same immunogen (thymocytes), a similar production method binding to similar epitopes. Thymoglobulin is more immunosuppressive than the previously used horse ATG. It results in a more prolonged period of lymphopenia, has a longer half-life, and has a higher affinity to human lymphocytes. To date, there have been only limited studies using rabbit ATG as first-line treatment for AA. In a small single center phase II study of 13 patients with AA and 12 patients with low-risk MDS, among the patients with AA, there were five complete responses and seven partial responses.24 A study from Brazil observed lower response rates when comparing patients treated by rabbit ATG with historical controls treated with horse ATG,25 whereas a Spanish group showed similar results in 79 patients.26 A comparative NIH study of horse (ATGAM) versus rabbit ATG (Thymoglobuline) is awaiting completion. A large prospective randomized study from China, with four arms, showed no benefit from growth factors added to horse ATG + CSA, confirmed that the combination of horse ATG + CSA was superior to horse ATG alone and superior to a different rabbit ATG preparation in combination with CSA. This ATG is only available in Europe and is generated by stimulating the animals with T-cell acute lymphoblastic leukemia blasts from the Jurkat cell line instead of thymocytes.14
Different brands of antithymocyte globulin
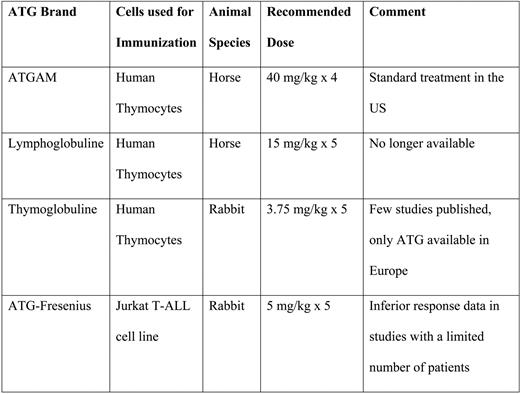
T-ALL indicates T-cell acute lymphoblastic leukemia.
ATG is given for 5 days as a daily intravenous infusion over 12 to 18 hours through a central venous catheter. There is a pronounced first-dose effect, with fever and rigors that will respond to steroids and reduction of infusion speed. Corticosteroids (1 mg/kg) and acetaminophen are given prior to each daily dose of ATG. Steroids are to prevent serum sickness and are tapered slowly over 4 weeks. Steroids do not contribute to response in AA patients, and prolonged treatment is to be avoided. Serum sickness typically occurs between days 7 and 14 from the start of ATG treatment. Symptoms include myoarthralgia, rash, fever, proteinuria, and platelet consumption. Oral CSA at 5 mg/kg/day may be started with ATG. We usually aim for CSA blood level between 150 and 250 μg/L, although there are no data on optimal levels in this disease. An Italian study showed reduced risks of relapse with prolonged CSA treatment; this has to be balanced against the side-effect profile of long-term CSA administration.27
The decision whether to use ATG in older patients can be difficult and requires careful assessment and discussion of the risks with the patient. For older patients, the response rate and survival rate are lower, compared with younger patients. The response rate for patients aged > 60, 50 to 59, and < 50 years is 37%, 49%, and 57%; 5-year survival is 50%, 57%, and 72%, respectively. For patients aged > 70 years, the 10-year survival is 33%, compared with 60% for those aged between 50 and 70 years.28,29 Although there is no upper age limit for ATG treatment, consideration for treatment should be preceded by medical assessment to exclude significant comorbidities. CSA treatment alone may be considered. The current EBMT treatment algorithm proposes to treat hospitalized patients who are severely ill by ATG + CSA, if considered to be tolerable considering the comorbidity profile, whereas to start newly diagnosed patients who are well and in an outpatient setting with CSA alone.
Other Immunosuppressants
High-dose cyclophosphamide without stem cell support is used by the Johns Hopkins Group as treatment for patients with newly diagnosed AA with roughly comparable response rates in newly diagnosed patients, compared with ATG + CSA.30 A prospective randomized study comparing this against ATG and CSA was terminated early because of excess deaths and fungal infections in the cyclophosphamide arm.31 Therefore, high-dose cyclophosphamide without stem cell support could not be recommended as first-line, in light of the data given. Its place, if any, in second-line or third-line treatment is not defined and has to be compared with alternative donor transplant strategies, other immunosuppressive strategies, and treatment by supportive care alone.
Mycophenolate mofetil inhibits the proliferation of B and T lymphocytes, and has been used in organ transplantation and autoimmune disorders. The EBMT WPSAA has recently performed a pilot study of 17 refractory patients without response.32 A study from the NIH showed no improvement in response or reduction in relapse after ATG + CSA when mycophenolate mofetil was added.33
Alemtuzumab (Campath-1H) is currently being investigated for refractory AA in prospective trials at the NIH and retrospectively by the EBMT, with a response rate of about 60% in a limited cohort of 35 heterogeneous patients.34
It is the group at the NIH who has the merit of initiating new studies trying to improve results of immunosuppressive treatment beyond what has been achieved by ATG + CSA more than 20 years ago. Recent improvement in outcome is probably more due to improved supportive care than to novel concepts of immunosuppressive treatment. A recent study adding sirolimus to ATG + CSA has not shown improved results35 ; on the other hand, there have been interesting response rates reported with daclizumab, an antibody directed against the interleukin-2 receptor,36 in patients with disease of moderate severity.
Supportive Care
Transfusional Support
Red cell and platelet transfusions are essential for patients with AA to maintain safe blood counts. Platelet transfusions should be given prophylactically when platelet count is < 10 × ·109/L or < 20 × ·109/L in the presence of fever. A common problem in multitransfused patients with AA is that they may develop alloimmunization to leukocytes present in red cell and platelet transfusions by generating anti HLA- (or non-HLA) antibodies. This can result in platelet refractoriness, as well as an increased risk of graft rejection after allogeneic BMT. Apart from transfusional support, practical measures to help prevent bleeding include dental hygiene, oral tranexamic acid, and control of menorrhagia with progestagens. Although there are no data on transfusion-induced GVHD in recipients of IST, experts recommend to universally use irradiated blood products during and after ATG therapy.37 There is, however, no consensus for how long after treatment to maintain this recommendation.
Infection Prevention and Treatment
Infectious complications in patients with SAA have been reviewed recently.38 The risk of infection is determined by the neutrophil counts. There is a wide variability in susceptibility to infectious complications. There is also an important difference between patients with a very low, but stable, neutrophil count (eg, 0.1–0.2 × 109/L) that may be sufficient to protect from most infections and patients with no neutrophils at all in their blood smear. Patients with AA are at risk of bacterial and fungal infections. Aspergillus infections have a very high mortality in patients with SAA and vSAA because of prolonged and severe neutropenia. AA patients who are severely neutropenic should ideally be cared for in isolation when in the hospital and should receive prophylactic antibiotics, antifungals, and regular mouth care (including antiseptic mouthwash).
As for all neutropenic patients, fever will require immediate hospitalization and treatment before the results of bacterial investigations are available. The local hospital guidelines for treatment of febrile neutropenia should be followed. This may include a combination of aminoglycosides and a β-lactam antibiotic, the exact choice depending on local hospital microbiologic sensitivity/resistance patterns. The duration of neutropenia, the patient's infection history, and recent antibiotics will also influence the choice of antibiotic, including the early introduction of broad-spectrum antifungals. Early use of an appropriate lipid formulation of amphotericin or one of the newer antifungal agents, such as Voriconazole or Caspofungin, should be considered in AA patients who may need prolonged treatment. Pulmonary infiltrates and sinus infection should be taken as indicators of likely fungal infection in patients with SAA. There have been no controlled studies evaluating the use of G-CSF or other hemopoietic growth factors in the treatment of severe infection in patients with AA. A short course of subcutaneous G-CSF at a dose of 5 μg/kg/day may be considered in neutropenic infection, if the patient has not been proven to be refractory to growth factors. G-CSF may produce a temporary neutrophil response, but usually only in those patients with residual marrow granulocytic activity. If there is no response by 1 week, it is reasonable to discontinue the drug.
Growth Factors
The rationale for using G-CSF after ATG + CSA is to attempt to reduce the risk of infection during the 3 months before neutrophil response is expected and to possibly improve response. However, prolonged use of growth factors may increase the risk of late clonal disorders, as shown by a retrospective EBMT WPSAA study.39 No study has ever shown an increase in trilineage response by the use of G-CSF. In a prospective Japanese study, the risk of relapse after response was decreased in the G-CSF arm. In a recent EBMT study, the association of ATG + CSA with G-CSF was associated with higher neutrophil counts, and less infection and hospitalization for the duration of G-CSF administration.19 Given these conflicting data, the EBMT WPSAA currently recommends to limit the use of G-CSF after ATG + CSA to patients with neutropenic infection.
Androgens
Androgens were used extensively in the treatment of AA for many decades before the availability of immunosupressants. In some patients, oxymetholone can stimulate erythropoiesis and rarely can produce a trilineage response; recent work has shown that androgens increase telomerase by indirect upregulation of the TERT (telomere reverse transcriptase) promoter.40 In combination with ATG, they increase response, but are hepatotoxic. Because of virilization, they are often unacceptable to women. The value of androgens in this disease, especially in refractory patients who are not candidates for alternative donor transplantation, needs to be reassessed in the current era.
Iron Chelation
Iron overload can cause problems in heavily transfused patients. Subcutaneous desferrioxamine should be started when serum ferritin is > 1000 μg/L, although evidence for this recommendation is lacking. This also needs to be assessed on an individual basis, in view of the risk of local hemorrhage and infection from subcutaneous injections. Alternatives are the oral iron chelator deferiprone, but this drug is associated with a risk of agranulocytosis. The novel oral iron chelator deferasirox is available for use in transfusion-dependent anemia. There is not sufficient data to assess the cytopenia risks associated with deferasirox treatment in AA patients, case-by-case decisions have to be made. For patients with iron overload with response to ATG + CSA or to BMT, venesection is the standard way to remove iron.
Patients with AA should be followed indefinitely to monitor for relapse and later for clonal disorders, such as MDS, leukemia, PNH, and solid tumors.
Disclosures
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Off-label drug use: None disclosed.
Correspondence
Jakob R. Passweg, MD, MS, Hematology Division, Geneva University Hospital, Rue G Perret-Gentil 4, 1211 Geneva 14, Switzerland; Phone: +41 22 3723958; Fax: +41 22 3727288; e-mail: Jakob.passweg@hcuge.ch
