
Abstract
von Willebrand disease (VWD) is the most common autosomally inherited bleeding disorder. The disease represents a range of quantitative and qualitative pathologies of the adhesive glycoprotein von Willebrand factor (VWF). The pathogenic mechanisms responsible for the type 2 qualitative variants of VWF are now well characterized, with most mutations representing missense substitutions influencing VWF multimer structure and interactions with platelet GPIbα and collagen and with factor VIII. The molecular pathology of type 3 VWD has been similarly well characterized, with an array of different mutation types producing either a null phenotype or the production of VWF that is not secreted. In contrast, the pathogenetic mechanisms responsible for type 1 VWD remain only partially resolved. In the hemostasis laboratory, the measurement of VWF:Ag and VWF:RCo are key components in the diagnostic algorithm for VWD, although the introduction of direct GPIbα-binding assays may become the functional assay of choice. Molecular genetic testing can provide additional benefit, but its utility is currently limited to type 2 and 3 VWD. The treatment of bleeding in VWD involves the use of desmopressin and plasma-derived VWF concentrates and a variety of adjunctive agents. Finally, a new recombinant VWF concentrate has just completed clinical trial evaluation and has demonstrated excellent hemostatic efficacy and safety.
Introduction
Our knowledge of von Willebrand disease (VWD) pathogenesis and the subsequent application of this information to benefit VWD diagnosis and therapy has advanced substantially over the past 25 years. After the immunologic distinction between von Willebrand factor (VWF) and factor VIII (FVIII) in the 1970s, the gene for VWF was cloned by 4 groups in 1985,1-4 and thus began an era of the integration of this knowledge into studies of disease pathogenesis, diagnosis, and treatment.
VWD epidemiology and classification
VWD is the most common autosomally inherited bleeding disorder, resulting in significant bleeding symptoms in ∼ 1 in 1000 subjects,5 although prevalence estimates ranging from 1%6 to 1 in 10 0007 have also been reported in the literature. The disease shows no geographical or ethnic predilection, but although both sexes inherit mutant VWF alleles with equal frequency, females outnumber males by approximately 2:1 in most VWD populations, presumably because of the burden of excessive mucocutaneous bleeding in reproductive age women.
The classification of VWD has remained relatively unchanged for the past decade.8 Type 1 VWD, a mild to moderate reduction in functionally normal VWF, constitutes 65% to 80% of cases; type 2 disease, involving the expression of functionally abnormal VWF, occurs in 20% to 35% of patients; and type 3 disease, the virtually complete absence of VWF, affects ∼ 1 in 1 million people depending upon the population structure and likelihood of inheritance of recessive alleles (Table 1).

The VWF gene and protein
The 175-kb VWF gene is located on the short arm of chromosome 12 and comprises 52 exons. The VWF gene sequence is replicated in part by a partial VWF pseudogene on chromosome 22. This evolutionary remnant recapitulates exons 23-34 of the VWF gene with 3% variance, a fact that significantly complicates the genetic analysis of this central region of the VWF gene.
The 9-kb VWF transcript encodes a pre-pro-VWF protein of 2813 amino acids. The protein undergoes extensive posttranslational modifications, including the removal of leader and propeptide sequences, dimer and eventual multimer generation, and the addition of many N-linked and O-linked carbohydrate structures. A recently revised annotation of the VWF protein structure indicates that whereas the platelet- and collagen-binding A domains of the protein form globular-like structures, a series of repetitive VWC domains toward the C-terminus provide the protein with increased length and flexibility, thus facilitating the transition between compact and extended conformations under conditions of shear stress in the vasculature (Figure 1).9

Diagram representing the revised annotation of the VWF mature subunit structure. This annotation, derived from electron microscopy analysis, demonstrates that the VWF D assemblies are composed of 4 smaller modules: VWF, 8-cysteine (C8), trypsin-like inhibitor (TIL), and E or fibronectin type 1-like modules (E). The previous B and C domains are now re-annotated as 6 tandem VWF C domains. The electron micrograph image of the D1 assembly shown here is from Zhou et al.9 As indicated, there is growing evidence that VWF interacts with a large number of ligands with a range of biological functions. VWFpp indicates VWF propeptide; OPG, osteoprotegerin; PSGL-1, P-selectin glycoprotein ligand-1; β2GPI, beta2 glycoprotein 1; and TSP1, thrombospondin 1.
Diagram representing the revised annotation of the VWF mature subunit structure. This annotation, derived from electron microscopy analysis, demonstrates that the VWF D assemblies are composed of 4 smaller modules: VWF, 8-cysteine (C8), trypsin-like inhibitor (TIL), and E or fibronectin type 1-like modules (E). The previous B and C domains are now re-annotated as 6 tandem VWF C domains. The electron micrograph image of the D1 assembly shown here is from Zhou et al.9 As indicated, there is growing evidence that VWF interacts with a large number of ligands with a range of biological functions. VWFpp indicates VWF propeptide; OPG, osteoprotegerin; PSGL-1, P-selectin glycoprotein ligand-1; β2GPI, beta2 glycoprotein 1; and TSP1, thrombospondin 1.
Pathogenesis of VWD
Over the past 25 years, significant progress has been made in our knowledge of the molecular pathogenesis of VWD, with particularly detailed understanding of the mechanisms underlying type 2 and 3 disease (Table 1).
Pathogenic mechanisms responsible for type 2 VWD
Type 2A VWD
This loss of platelet–dependent function variant of VWD comprises 20% to 25% of VWD cases in most series. The key hemostatic test findings are low VWF antigen (VWF:Ag) and VWF ristocetin cofactor activity (VWF:RCo) levels with a RCo:Ag ratio of < 0.6 in association with a VWF multimer profile showing loss of high-molecular-weight multimers (HMWMs) and sometimes intermediate-molecular-weight multimers. This pattern of results can also be seen in type 2B VWD and the critical differentiating test is the ristocetin-induced platelet agglutination test that shows a lack of response in type 2A disease and hyperresponsiveness in 2B VWD. The lack of HMWMs in type 2A disease is due to a range of biosynthetic and post-biosynthetic abnormalities that influence the generation and proteolysis of the protein.10 Missense substitutions in the VWF propeptide, D′/D3 and A2 domains, and in the C-terminal cysteine knot domain can all interfere with HMWM assembly, and missense substitutions in the A2 domain can facilitate accelerated ADAMTS13-mediated proteolysis at the Tyr1605-Met1606 cleavage site in this domain.11
Type 2B VWD
This gain-of-function variant is the result of missense mutations in the GPIbα-binding A1 domain of VWF. The phenotype is transmitted as a highly penetrant dominant trait, and clinical and mouse model evidence indicates that the bleeding severity and accompanying thrombocytopenia is related predominantly to the specific type 2B mutation inherited.12-14 In addition, acquired influences such as acute stress and pregnancy, in which the levels of mutant protein are increased, will also result in worsening of the in vivo platelet clumping and thrombocytopenia, thus aggravating the risk of bleeding.12 This disorder has a genocopy in platelet-type VWD in which gain-of-function mutations in the GPIbα gene result in enhanced binding to VWF.15 The 2 conditions can be differentiated by either plasma- or platelet-mixing studies or more definitively by genetic analysis.
Type 2M VWD
This VWD variant is characterized by loss-of-function VWF mutations affecting either GPIbα or collagen binding. The GPIbα-binding mutants demonstrate reduced VWF:RCo/VWF:Ag ratios of < 0.6 in association with a normal multimer pattern, whereas the collagen-binding variants may only show abnormalities in specific collagen-binding assays. The GPIbα-binding substitutions are located in the A1 domain and collagen-binding variants have been identified in the A3 domain and, more recently, in the A1 domain. Although the “classical” type 2M phenotype associated with poor GPIbα binding and unresponsiveness to desmopressin is well recognized, the status of the collagen-binding mutants remains less clear. Earlier reports of poor binding to type I and III collagens were associated with missense substitutions in the A3 domain,16,17 but recent evidence suggests that substitutions in the A1 domain may impede binding to type VI collagen and also result in a mild bleeding phenotype.18
Type 2N VWD
This variant presents as an autosomal form of mild/moderately severe FVIII deficiency. In contrast to the other type 2 variants of VWD, type 2N disease is transmitted in a recessive fashion with a variety of homozygous and compound heterozygous genotypes, resulting in FVIII levels between 5% and 40%.19 In all instances, the FVIII levels are disproportionately low compared with VWF. All of the mutations responsible for this phenotype are located either within the N-terminal D′/D3 assembly FVIII-binding region of VWF (> 95% of cases) or at the furin cleavage site for removal of the VWF propeptide.
Type 3 VWD
The hemostasis phenotype for type 3 disease demonstrates a very low (< 5%) to undetectable level of VWF:Ag and VWF:RCo and a FVIII:C that is usually < 10%.20 The disease is transmitted as either a recessive trait (normal parents) or through the inheritance of 2 mutant codominant alleles (both parents have type 1 VWD).21 The > 110 type 3 VWD cases that have been genetically characterized show a range of VWF mutations, from large VWF deletions through a miscellany of null mutations to missense mutations that prevent VWF biosynthesis and secretion. Although initial studies of the infrequent cases of type 3 VWD developing alloantibodies to VWF showed an association with VWF deletion mutations,22,23 there has been no systematic confirmation of this observation.24
Type 1 VWD
Type 1 disease comprises 65% to 75% of VWD cases in most series. The phenotype in type 1 disease is extremely heterogeneous, with VWF levels ranging from 5% to 40% depending on the molecular pathogenesis. Pathogenetic mechanisms in type 1 VWD most often involve “classical” dominant effects with mutation-specific penetrance, although a dominant-negative effect is observed in some cases.
Until recently, the molecular pathology responsible for this condition was unknown. Four molecular epidemiological studies of ∼ 500 index cases of type 1 VWD have now indicated that candidate VWF mutations are present in ∼ 65% of index cases and that ∼ 70% of these sequence variants represent missense substitutions.25-28 Furthermore, the more severe the VWF deficiency, the greater the likelihood of finding a clear VWF mutation. To date, the pathophysiological mechanisms resulting from these VWF mutations include a full range of abnormal functions from defective transcriptional activation,29 aberrant splicing, and various abnormalities of subcellular targeting, storage and secretion30 to a predominantly accelerated clearance phenotype.31 This latter group of patients can be most readily identified through an increase in the VWF propeptide/VWF:Ag ratio that can be used as a surrogate for VWF survival.32 Recent studies using patient-derived circulating endothelial progenitor cells appear to have the potential of providing more detailed information concerning the biosynthetic defects operating in these cases.33,34
With the recent evidence that 35% of index cases of type 1 VWD have no identifiable VWF mutations, the search for additional genetic modifiers of this phenotype has just begun. One well-documented contributor to quantitative variation of VWF is the ABO blood group, with VWF levels being ∼ 25% lower in group “O” subjects.35 This association was resoundingly confirmed in a recent genome-wide association meta-analysis that also identified 6 novel loci that influence both VWF and FVIII plasma levels.36 The biological plausibility of these loci playing a role in regulating the plasma levels of these proteins is further supported by the fact that 2 of the genes encode proteins involved in vesicular trafficking and exocytosis (syntaxin-binding protein 5 and syntaxin 2) and 3 of the genes encode lectin or scavenger clearance receptors (scavenger receptor class A member 5, stabilin 2, and C-type lectin type 4 member M). Further evidence confirming the involvement of these proteins in regulating VWF levels is just now beginning to appear.37 Finally, beyond the consideration of VWF, the coexistence of other mild bleeding disorders might also modify the clinical phenotype in these patients.
Diagnostic approaches to VWD
The diagnosis of VWD continues to involve the constellation of clinical symptoms of excessive mucocutaneous bleeding, coagulation studies consistent with quantitative and /or qualitative VWF abnormalities, and usually a family history of the disease.
Utility of bleeding assessment tools
In the past decade, there has been a resurgence of interest in developing quantitative bleeding assessment tools (BATs).38 These tools have been evaluated predominantly in disorders of mucocutaneous hemostasis, with extensive use in studies of VWD.39 In these studies, there has been a good correlation among the VWD subtype, VWF:Ag level, and the bleeding score, with the highest scores in type 3 disease and intermediate scores in type 2 subtypes.39,40 The application of BATs is especially helpful for the following reasons: (1) they have a high negative predictive value in screening individuals for a bleeding disorder, (2) they are a means of rationalizing more intense laboratory investigation of bleeding, and (3) they serve as a quantitative, short-form approach for communicating bleeding severity among health care providers. Although the International Society on Thrombosis and Haemostasis (ISTH) has now developed a widely used BAT, it is increasingly recognized that one BAT may not be suitable in all bleeding situations and that, in these circumstances, alternate tools will be required to assess the clinical problem objectively.
Coagulation test phenotype in VWD (Table 2)
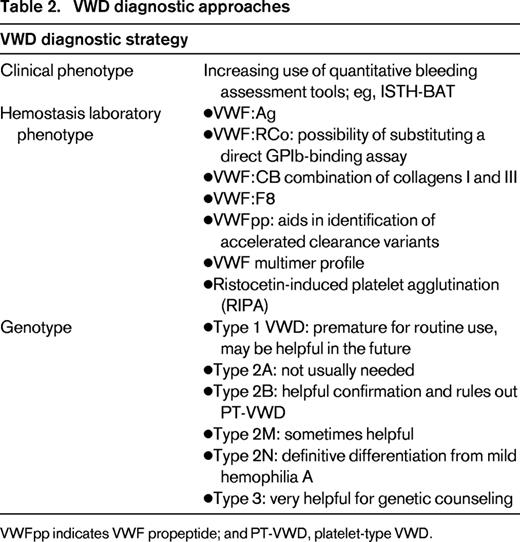
Central to the confirmation of VWD diagnosis are appropriately standardized measurements of VWF:Ag and VWF platelet-dependent function. This latter analysis currently involves testing for VWF:RCo, but this test is notoriously difficult to standardize and is relatively insensitive at VWF levels < 10%. Therefore, the recent development of assays to quantify direct binding of VWF to platelet GPIbα appears to offer significant advantages,41 although a more comprehensive evaluation of different qualitative VWD variants must first be completed to ensure that the assays are sensitive to all appropriate structural changes.42
Another complicating issue that has arisen in the interpretation of the platelet-dependent functional assay for VWF is the interference in the VWF:RCo assay with a polymorphism at codon 1472 (D1472H).43 This polymorphic variant is located immediately adjacent to the distal binding site for ristocetin in the VWF A1 domain and, despite demonstrating lower VWF:RCo/VWF:Ag ratios, patients heterozygous for this polymorphism have not been found to exhibit increased bleeding.44
Confirmation of the diagnosis of type 1 VWD with coagulation test performance is inevitably complicated by several physiological factors influencing the plasma levels of VWF. Furthermore, the nature and severity of bleeding in type 1 VWD is variable and is not distinguishable from other mucocutaneous bleeding disorders. In the laboratory, it is important to remember that VWF is an acute-phase protein prone to the transient fluctuations inherent with this group of proteins. Therefore, in patients with clear clinical evidence of a bleeding phenotype, quantification of VWF levels should be evaluated at least twice to ensure that true baseline values are obtained. Second, the gradual increase of VWF levels with age also complicates the interpretation of results from individuals with mildly reduced plasma VWF levels, in whom protein levels are likely to increase into the normal range over several years. Although many (most) of these mild-type 1 VWD patients will have corrected their VWF levels by age 50, it remains unclear whether their original bleeding tendencies are also rescued.
In addition to determining the platelet-binding function of VWF, there is now good reason to add a specific assay to quantify the collagen-binding potential of the protein. Several families have now been described in whom the only defect in VWF function is reduced collagen binding, so these cases will be missed with the standard VWF testing panel. The question remains as to whether testing should be performed with type I and III collagen only (assessing binding through the A3 domain) or if binding to collagen type VI (mediated by the A1 domain) should also be evaluated.45 Resolution of this dilemma will require larger study populations and additional genetic analysis of the A1 and A3 domains.
The most demanding diagnostic test for VWD is the VWF multimer analysis, an investigation that challenges even the most seasoned laboratory technologist. Robust evidence of the loss of HMWMs is important in the diagnosis of type 2A and 2B VWD, but the VWF multimer profile cannot be used to differentiate between these 2 variants. This must involve the demonstration of hypersensitivity to low-dose ristocetin for type 2B mutants in the ristocetin-induced platelet agglutination test. This diagnostic consideration should also take into account the type 2B genocopy, platelet-type VWD, in which the gain-of-function causative mutations are located in the GPIBA gene.15 Although a pragmatic substitute for multimer analysis is not envisaged in the near future, with the exception of the infrequent type 2M collagen-binding mutants, the collagen-binding capacity of VWF provides a useful surrogate measure for the presence of HMWMs and thus further supports the rationale for performing this assay.
Role of genetic analysis in VWD
Now, 28 years since the cloning of the VWF gene, there is a growing role for the integration of genetic testing in VWD. The best examples of the utility of genetic diagnosis are in type 2 and 3 disease. In light of the fact that the mutations responsible for types 2B, 2M, and 2N VWD are all localized within discreet regions of the VWF gene, and in each instance the disease phenotype may not be definitive, genetic testing to confirm these VWD subtypes will often be useful (Figure 2). Similarly, given the severe phenotype of type 3 VWD, genetic prenatal diagnosis of this variant provides results for families and their physicians to make informed decisions about family planning and obstetric management issues.

Figure illustrating the location of mutations resulting in the various VWD subtypes. Types 1 and 3 VWD are caused by different types of mutation throughout the VWF sequence. In contrast, the type 2 VWD mutations are localized to distinct functional domains of VWF, affecting multimer structure (2A), binding to FVIII (2N), platelets (2B and 2M), and collagen (2M).
Figure illustrating the location of mutations resulting in the various VWD subtypes. Types 1 and 3 VWD are caused by different types of mutation throughout the VWF sequence. In contrast, the type 2 VWD mutations are localized to distinct functional domains of VWF, affecting multimer structure (2A), binding to FVIII (2N), platelets (2B and 2M), and collagen (2M).
In contrast to the utility of genetic testing in type 2 and 3 VWD, the rationale for incorporating VWF genotyping as an adjunctive diagnostic strategy in type 1 disease is much less clear. With candidate VWF mutations not being found in 35% of type 1 VWD index cases and with a growing appreciation of problems in the differentiation between pathogenic mutations and neutral polymorphisms,28 the routine use of genetic analysis to evaluate diagnostically challenging cases of type 1 VWD is difficult to justify. Most of these missing mutations are in cases with mild phenotypes in whom diagnostic certainty is often challenging. In the meantime, additional research needs to be performed to identify other genetic factors with an influence on plasma VWF levels that may be of sufficient importance to incorporate into genetic testing algorithms for this phenotype. Unfortunately, the inevitable fact remains that borderline cases of VWF deficiency will continue to challenge the definitive assignment of disease status.
Advances in the treatment of VWD
Little has changed in the landscape of VWD therapies over the past 2 decades (Table 3). In many cases of type 1 VWD, and in some cases of type 2A disease, the use of desmopressin will provide adequate hemostatic coverage to treat mucocutaneous bleeding and to prevent bleeding at the time of minimally invasive procedures.46-49 The use of this agent in type 2B, 2N, and 3 disease is usually not effective. All patients thought to be potential candidates for the use of desmopressin should undergo a therapeutic trial with measurements of VWF:Ag, VWF:RCo, and FVIII:C out to at least 4 hours after desmopressin administration to evaluate the possibility of accelerated clearance of the newly released protein. Adjunctive therapy with antifibrinolytic agents (ideally tranexamic acid) is also of significant benefit in VWD; in women with VWD experiencing menorrhagia, the use of an oral contraceptive or the levonorgestrel-releasing intrauterine device (Mirena) often produces excellent results.50
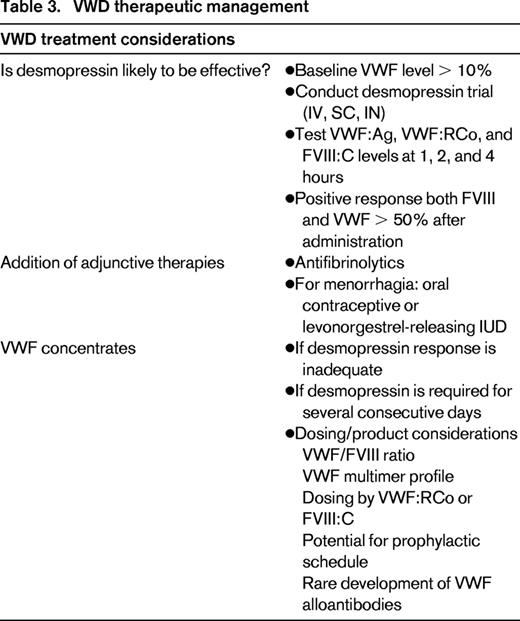
For patients not responding adequately to desmopressin or to the various forms of adjunctive agents, there is now a variety of VWF concentrates available for protein replacement therapy. All but one of these products represent plasma-derived VWF-FVIII concentrates with various VWF:FVIII ratios and multimer profiles that show minor differences.51 In the studies that have been published relating to the clinical efficacy and safety of these products, they all appear to provide satisfactory hemostasis and are not accompanied by serious adverse events. The use of VWF concentrates with very low FVIII content should be accompanied by the coinfusion of recombinant FVIII to enhance the treatment of acute bleeding episodes and to optimize surgical hemostasis. Any variances in multimer content of the products have not resulted in obvious differences in the clinical outcomes and the optimal dosing rationale and schedule for these concentrates is still not reconciled definitively. Although dosing in FVIII:C units for surgical hemostasis is recommended by some, there may be more justification for using VWF:RCo–based dosing to treat or prevent mucocutaneous bleeding.
The use of VWF-FVIII products for bleeding prophylaxis has been explored in a few studies, but even in type 3 disease, in which the need for this strategy is the most obvious to prevent recurrent musculoskeletal and mucosal bleeding, there is no consensus on the concentrate dose and administration schedule. Nevertheless, there is no doubt that extended concentrate prophylaxis is effective in some patients with these clinical problems.52
In the past couple of years, we have seen the initial clinical trial of a new recombinant VWF (rVWF) concentrate that has been administered in a 1.3:1 (VWF:RCo to FVIII:C) ratio with recombinant FVIII.53 In vitro analysis of this material shows that the rVWF displays a full array of large and ultra-large-molecular-weight multimers, as would be expected from a product that has not been exposed to ADAMTS13 proteolysis during production.
The clinical trial of this new concentrate has demonstrated excellent hemostatic efficacy and safety, with effective bleeding control and no evidence of immunogenicity. Detailed postinfusion studies show that ADAMTS13-mediated proteolysis of the infused rVWF is prompt and there has been no evidence of a microangiopathic state after administration.
Future of VWD clinical management
Although recent advances in our understanding of the pathophysiology of VWD have been significant, the diagnostic and therapeutic landscape has remained relatively unchanged for more than a decade. The increasing use of BATs and the incorporation of molecular analysis into laboratory testing algorithms for some VWD subtypes will enhance diagnostic capabilities, but aside from the introduction of the new rVWF concentrate, the therapeutic approaches for the treatment and prevention of bleeding have not changed since the 1990s. Although preclinical successes of gene therapy for VWD have been reported,54 there is no clear clinical rationale for the development of this therapeutic modality in this condition. What may be of more interest to both the VWD and hemophilia A communities would be the development of VWF molecules that exhibit longer half-lives. However, to achieve this goal, more basic information about normal VWF clearance mechanisms is required, a goal that might simultaneously provide more knowledge concerning factors that contribute to the qualitative trait of type 1 VWD.
This article was selected by the Blood and Hematology 2013 American Society of Hematology Education Program editors for concurrent submission to Blood and Hematology 2013. This article is reprinted with permission from Blood. 2013; Volume 122.
Acknowledgments
D.L. is the recipient of a Canada Research Chair in Molecular Hemostasis. His studies of VWD are supported by the Canadian Institutes of Health Research, the National Institutes of Health, and the Canadian Hemophilia Society.
Disclosures
Conflict-of-interest disclosure: The author has received research funding from Biogen-Idec, CSL-Behring, Baxter, and Bayer. Off-label drug use: None disclosed.
Correspondence
Dr David Lillicrap, Department of Pathology and Molecular Medicine, Richardson Laboratory, Queen's University, Kingston, ON, K7L 3N6, Canada; Phone: 613-548-1304; Fax: 613-548-1356; e-mail: dpl@queensu.ca.
