

Abstract
A relative wealth of new therapies for acute myeloid leukemia (AML) have led to a rapid shift in treatment paradigms for this disease. Understanding whom, when, and how to treat is more complex than ever before. Here we explore whom to treat with these available new therapies, focusing on special patient populations that include older adults, those with relapsed disease, and those with TP53-mutated AML. These high-risk subgroups are some of the most challenging to care for, but novel treatments are providing them with new hope.
Learning Objectives
Learn the indications for newly approved and emerging drugs in AML in challenging populations
Become familiar with a treatment algorithm for older, relapsed, and TP53-mutated AML patients
Introduction
The recent approval of a variety of novel therapies for acute myeloid leukemia (AML) has provided more treatment options for patients than ever before. However, identifying whom to treat, and how, can be challenging. Key elements in making these decisions include assessing patient characteristics and obtaining comprehensive AML profiling, including cytogenetic and molecular data. Even with this information, the optimal therapeutic path is not always clear. Here we highlight the complexities of selecting whom to treat with novel AML therapies.
CLINICAL CASE
An 86-year-old man with a past medical history of hypertension and gastroesophageal reflux disease developed leukocytosis, anemia, and thrombocytopenia. A bone marrow biopsy revealed 60% myeloblasts. Immunophenotypically, the blasts were CD34+, CD13+, and CD33+. He was diagnosed with AML. Next-generation sequencing showed mutations in ASXL1 and IDH1. Findings from the karyotype were normal.
With a median age of 68 years at the time of diagnosis, AML is primarily a disease of older adults.1 However, the incidence of AML not only increases with age but also becomes more difficult to treat and cure. Five-year overall survival (OS) for patients diagnosed between the ages of 60 and 64 is 22%, while that of patients diagnosed over the age of 80 is 1.3%.2 The advent of newer, less toxic treatments may help to improve this disparity.
Outcomes for older adults with AML are poor because of many complex reasons (Figure 1) First, patient factors such as comorbidities and decreased baseline performance status (PS) may prevent patients from receiving optimal therapy or put them at higher risk of complications. The number of comorbidities increases with age and correlates with an increase in AML-related and all-cause mortality.3 Older patients are also more likely to present with an ECOG PS of 2 or 3, and decreased PS is associated with an increase in early death.4 Older patients with decreased PS are more likely to experience early mortality than younger patients with a similar PS, indicating the complex interplay between these 2 factors.5,6
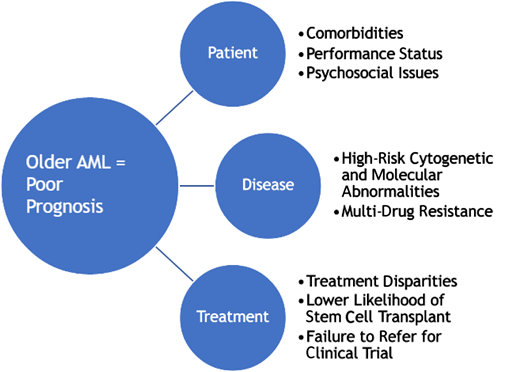
Second, disease-related factors also contribute to poorer outcomes in older patients. Such patients are more likely to have disease with high-risk chromosomal abnormalities (−5 or 5q−, −7 or 7q−, or 17p deletion), and the incidence of having high-risk mutations in genes such as ASXL1,RUNX1, and TP53 also increases with age.7 By European LeukemiaNet criteria, older patients more often have high-risk disease, and survival for these patients is decreased compared to younger patients with similarly high-risk disease.8,9 Older patients also more frequently have disease that is inherently chemotherapy-resistant due to overexpression of the MDR1 multidrug-resistance gene.10
Finally, several factors influence the type and intensity of treatments offered to older patients, leading to decreased survival. Older patients are less likely to be offered up-front treatment for AML and are less likely to undergo allogeneic stem cell transplant.11,12 This is despite the fact that studies have demonstrated that treatment of any intensity improves survival in this patient population.11 The reasons for these disparities include physician bias regarding the treatment of older patients, caregiver issues, and other socioeconomic inequities.
Given the urgent need to address disparities in outcomes for older individuals with AML, in 2020 the American Society of Hematology published guidelines for treating these patients.13 The guidelines are based on a systematic review of the literature and consider many of the previously discussed factors. Included is a recommendation to offer antileukemic therapy over best supportive care and to attempt intensive therapy when possible. As newer therapies continue to emerge, these guidelines must be adapted and modified, particularly with regard to intensity of treatment. Ultimately, optimal therapy for older adults with AML is that which provides the best depth of response, imparts the least amount of toxicity, and meets the goals of the individual patient.
Recent efforts to develop safer and more effective treatments for older adults with AML are beginning to pay off. Leading the way has been the US Food and Drug Administration (FDA)-approved frontline combination of azacitidine and venetoclax (AZA-VEN). This lower-intensity treatment was shown in the phase 3, multicenter, randomized, double-blind, placebo-controlled VIALE-A trial to improve OS when compared to azacitidine plus placebo (14.7 months vs 9.6 months; hazard ratio [HR], 0.66; 95% CI, 0.52-0.85; P < .001) in patients over 75 or in younger patients with significant comorbidities.14 Moreover, the composite complete remission (CR) rate was 66.4% for patients in the AZA-VEN group compared to 28.3% in the control group, and rates of red blood cell and platelet transfusion independence were 59.8% and 68.5%, respectively. Regarding safety, rates of grade ≥3 neutropenia and neutropenic fever were higher in the AZA-VEN group; however, 30-day mortality was similar between the 2 groups (7% with AZA-VEN and 6% with AZA-placebo).
Molecular subgroup analysis of the VIALE-A study suggests that mutations in IDH1 or IDH2 may confer a particularly favorable response to AZA-VEN. A pooled analysis of the phase 1b and phase 3 studies showed that CR/complete remission with partial hematologic recovery (CRh) for patients with an IDH1 mutation was 59% with AZA-VEN vs 9% with AZA-placebo. CR/CRh for patients with an IDH2 mutation was 80% with AZA-VEN vs 6% with AZA-placebo.15 This improvement in remission rates translated into an improvement in duration of response and OS. This differed from other molecular subsets, such as FLT3-mutated or TP53-mutated disease, where responses were better withAZA-VEN, but OS was not affected.
The oral IDH1 inhibitor ivosidenib is another FDA-approved frontline therapy for older patients with AML. This treatment was initially studied in a phase 1, multicenter, open-label, dose-escalation, dose-expansion study in patients with AML with an IDH1 mutation.16 The median age in the study was 76.5 years, and 56% of patients were over 75. The CR/CRh rate was 42%, with a median time to response of 2.8 months. The median follow-up was 23.5 months, with a median OS of 12.6 months. The utility of ivosidenib as a single agent is limited, but it may be a good option for patients unable to receive venetoclax or tolerate combination treatment. A study of azacitidine, venetoclax, and ivosidenib is underway (NCT03471260), and the results, if positive, will increase the value of this agent.
The phase 2 BRIGHT AML 1003 study assessed the combination of low-dose cytarabine and glasdegib, a hedgehog pathway inhibitor, vs low-dose cytarabine alone.17 The median age in the glasdegib arm was 77 and in the low-dose cytarabine arm, 75. The addition of glasdegib improved median OS (8.8 vs 4.6 months; HR, 0.51; 80% CI, 0.39-0.67; P = .0004). This led to the FDA approval of glasdegib plus low-dose cytarabine for the treatment of older patients with AML. However, given the other FDA-approved treatment options, which appear to be more efficacious and equally as safe, the clinical utility of this treatment is questionable. Subsequent subset analysis indicated slightly improved survival in patients with secondary AML as opposed to de novo disease.18 Though no head-to-head comparison exists, this survival was shorter than that of patients treated with AZA-VEN in VIALE-A.14,18
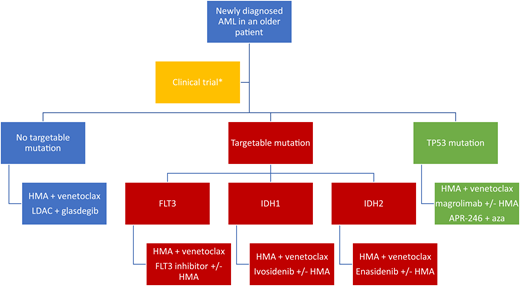
Numerous trials evaluating targeted therapies, combination therapies, and novel agents for the frontline treatment of older patients with AML are underway. In addition, geriatric assessment tools are being developed and evaluated with the hope of improving treatment selection, side effects, and patient quality of life. These advances will continue to have a positive impact on the lives of older patients with AML. (See Figure 2 for a treatment algorithm for older patients.)
CLINICAL CASE
An 81-year-old woman was treated with AZA-VEN for newly diagnosed AML. After 2 cycles, her disease went into CR. She remained on this treatment for 7 cycles before her disease relapsed. Repeat molecular testing showed a new FLT3-ITD mutation and a new mutation in IDH2.
In spite of the advances made in the first-line treatment of AML, approximately 50% of patients experience a relapse.19,20 The treatment options for relapsed or refractory (R/R) disease remain limited, and 5-year OS for these patients is approximately 10%.21 Outcomes after first-line treatment with a hypomethylating agent and venetoclax are particularly poor, with a median survival of 2.4 months.22 At the time of relapse, molecular testing should be repeated to assess for the presence of targetable mutations. Due to clonal evolution, previously identifiable targets may be lost, or the emergence of subclones may lead to the presence of new targets.23
Several targeted therapies have been approved for the treatment of R/R AML. For patients with FLT3-mutated disease, gilteritinib is a potent oral FLT3 inhibitor that can be used as a single agent. In the randomized phase 3 ADMIRAL study, gilteritinib improved OS when compared to investigator-choice chemotherapy (9.3 months vs 5.6 months; two-sided P < .001).24 About 34% of patients receiving gilteritinib had a CR/compelete remission with incomplete count recovery compared to 15.3% in the chemotherapy group (risk difference, 18.6 percentage points; 95% CI, 9.8-27.4). Given its modest efficacy as a single agent, gilteritinib is being studied in combination with other therapies in the relapsed and frontline setting. Early data on the combination of gilteritinib and venetoclax for relapsed FLT3-mutated AML look promising.25
The previously mentioned IDH1 inhibitor, ivosidenib, is also approved for the treatment of R/R AML with an IDH1 mutation. In a large, single-arm phase 1 study, ivosidenib was shown to be safe and well tolerated and to induce a CR or CRh in 30.4% of patients.26 Similarly, the IDH2 inhibitor enasidenib is approved for the treatment of R/R AML with a mutation in IDH2. This approval was based on the phase 1/2 study that showed a CR rate of 19.3% in this population.27 However, the phase 3 study for this drug failed to meet the primary OS end point.28 Combination studies with enasidenib are underway.
Finally, the somewhat controversial CD33-targeted antibody-drug conjugate gemtuzumab ozogamicin (GO) is also approved for patients with AML that is R/R. First approved in 2000, GO was voluntarily withdrawn from the US market in 2010 due to safety concerns. Reapproval was granted in 2017 after further review of the data. In the ALFA 9801 trial, GO, which was given as a single agent or in combination with chemotherapy to patients with R/R disease, demonstrated a 39% CR rate.29 Pooled analysis of the data from 3 other phase 2 studies showed a slightly lower overall remission rate of 26%.30 There is interest in combination therapy with GO and studies in this area are ongoing.
Although these agents represent progress for the treatment of patients with R/R AML, response rates and long-term survival are still limited, and clinical trials remain the preferred option at first relapse or after the use of targeted therapies. Many novel agents are under investigation, including small molecule inhibitors, immunotherapies, and combination therapies, and new candidates for targeted treatments continue to be identified. (See Figure 3 for a treatment algorithm for patients with relapsed disease.)

CLINICAL CASE
A 78-year-old woman with a past medical history of hypertension developed leukocytosis, anemia, and thrombocytopenia. A bone marrow biopsy revealed 60% myeloblasts. Immunophenotypically, the blasts were CD34+, CD13+, and CD33+. She was diagnosed with AML. Next-generation sequencing showed a mutation in TP53.
TP53, an essential tumor suppressor gene, is mutated in up to 10% of AML cases.31 It is found more frequently in therapy-related and complex-karyotype AML. This mutational status is an important prognostic factor that consistently corresponds to extremely poor outcomes, including low response rates to traditional cytotoxic chemotherapy and rare instances of long-term survival after allogeneic transplantation.32,33
Unfortunately, the novel agents approved for the treatment of AML, including therapy related and complex karyotype, have not led to significant improvement in the survival of patients with TP53-mutated AML. For example, a 2018 study evaluated this subgroup of patients in the registration trial of CPX-351 vs 7 + 3 in older adults with newly diagnosed high-risk or secondary AML.34 Patients with the mutation had a median survival of 5.7 months in the CPX-351 arm and 5.1 months in the 7 + 3 arm, demonstrating no benefit. A subsequent small study by Kim et al,35 which looked at the real-world use of CPX-351 in 53 patients, 30% of whom had TP53-mutated AML, showed more encouraging results in this subset, with an overall response rate (ORR) of 57% (8/14) and a 63% measurable residual disease negativity rate by next generation sequencing. However, these retrospective data should be interpreted cautiously. Skepticism about the efficacy of CPX-351 for TP53-mutated AML remains.
The previously discussed VIALE-A trial showed significantly higher rates of composite remission for patients with TP53-mutated AML who received azacytadine and venetoclax than those in the control group (55.3% vs 0%, respectively; 95% CI, 38.3-71.4; P < .001).14 However, this did not translate to an increase in OS. Disappointingly, combining venetoclax with 10 days of decitabine improved neither response rates nor OS.36 The addition of venetoclax to more aggressive therapy (FLAG-IDA) also failed to show improvement in the TP53-mutated AML subgroup.37
Hope for this poor-risk population likely lies in the use of novel agents. For example, magrolimab is a first-in-class macrophage immune checkpoint inhibitor targeting CD47. CD47 is a “do not eat me” signal overexpressed in multiple cancers, including AML.38 Its activation leads to macrophage immune evasion. Magrolimab eliminates tumor cells through macrophage phagocytosis. Data were presented at ASH 2020 from a trial using magrolimab plus azacitidine in patients with newly diagnosed AML who were ineligible for intensive chemotherapy. The study primarily enrolled patients with TP53-mutated AML (65%, as they were preferentially enrolled after an early protocol amendment).39 The combination induced a 71% ORR and 48% CR rate in this high-risk subgroup. Moreover, the median OS for these patients was 12.9 months. Based upon these data and the high unmet need in this population, a randomized phase 3 trial of magrolimab plus azacitidine vs AZA-VEN or intensive induction as a frontline therapy for TP53-mutant AML is preparing to begin recruitment (NCT04778397).
Another novel agent that targets TP53 more specifically is APR-246, a methylated PRIMA-1 analogue. It is a first-in-class small molecule that selectively induces apoptosis in TP53 mutant cancer cells.40 The agent is spontaneously converted into the active species methylene quinuclidinone, which covalently binds to cysteine residues in mutant p53, thereby producing thermodynamic stabilization of the protein and shifting equilibrium toward a functional conformation. Two early phase studies were recently published assessing the combination of APR-246 and azacitidine. A phase 1b/2 study in patients with TP53-mutated myelo dysplasic syndrome (MDS) or low-blast percentage AML showed the treatment to be safe and well tolerated.41 The ORR was 88%, with a CR rate of 61% for the MDS cohort and 50% for the AML; median OS was 10.8 months (95% CI, 8.1-13.4). A similar phase 2 study of APR-246 plus azacitidine included patients with MDS, low-blast AML, and AML with blasts >30%.42 Response rates and OS for the MDS and low-blast AML cohorts were similar to the previously discussed trial. However, response rates and survival in patients with AML with >30% blasts were lower (ORR 50%, CR 0%, OS 3 months). These studies are encouraging for patients with MDS or low-blast AML but suggest that triplet therapy or other combinations with APR-246 should be explored in AML with higher blast counts. One such study looking at APR-246 plus azacitidine and venetoclax is ongoing (NCT04214860).
Finally, the ongoing trial GLAD-AML (NCT03798678) addresses this poor-risk population in a randomized phase 2 study combining glasdegib with DEC5 or DEC10 in patients with newly diagnosed poor-risk AML.
Conclusion
Understanding who will benefit from current and future novel AML therapies is an evolving area. Patient age and fitness, disease biology, and treatment mechanism of action must all be taken into consideration when choosing whom to treat and how. In general, even low-intensity treatment provides a survival benefit over best supportive care to patients of all ages and molecular and cytogenetic subgroups. Trials looking to build on recent improvements in outcomes are ongoing, including some with doublet and triplet therapy as well as others looking at drug sequencing, MRD eradication, and maintenance.
Conflict-of-interest disclosure
Lindsay Wilde: no conflicts to disclose.
Margaret Kasner: research funding: Astellas, Diachi, Gilead, Jazz, Telios, Ono, Otsuka, Pfizer; honoraria: Kite, Jazz, Ono.
Off-label drug use
Lindsay Wilde: no discussion of off-label drug use outside of the setting of clinical trials.
Margaret Kasner: no discussion of off-label drug use outside of the setting of clinical trials.
