

Abstract
Among indolent non-Hodgkin lymphomas (iNHLs), the analysis of measurable/minimal residual disease (MRD) has been extensively applied to follicular lymphoma (FL). Treatment combinations have deeply changed over the years, as well as the techniques to measure MRD, which is currently evaluated only in the setting of clinical trials. Here, we discuss the evidence on the role of molecular monitoring in the management of FL. Mature data support the quantification of molecular tumor burden at diagnosis as a tool to stratify patients in risk categories and of MRD evaluation at the end of treatment to predict progression-free survival and overall survival. Moreover, MRD deserves further studies as a tool to refine the clinical/metabolic response and to modulate treatment intensity/duration. Patients with a higher relapse probability can be identified, but the relevance of continuous molecular follow-up should be clarified by kinetic models of MRD analysis. Being the BCL2/heavy chain immunoglobulin gene hybrid rearrangement detectable in about 50% to 60% of advanced FL and in 30% of positron emission tomography/computed tomography–staged localized FL, technical advancements such as next-generation sequencing/target locus amplification may allow broadening the FL population carrying a molecular marker. Droplet digital polymerase chain reaction can better quantify MRD at low levels, and novel sources of DNA, such as cell-free DNA, may represent a noninvasive tool to monitor MRD. Finally, MRD in other iNHLs, such as lymphoplasmacytic lymphoma/Waldenström macroglobulinemia and marginal zone lymphoma, is beginning to be explored.
Learning Objectives
Describe the accumulating data on MRD monitoring in patients with advanced and localized FL in the immunochemotherapy and chemo-free era
Understand how MRD might be used in the clinical management of patients with FL
Discuss how new technologies could overcome the current limitations in order to widely apply MRD to patients with FL and to other indolent NHLs
Introduction
Indolent non-Hodgkin lymphomas (iNHLs) often spread to the bone marrow (BM) and/or peripheral blood (PB) and can be monitored through the identification at diagnosis of a disease marker to be followed during treatment.1 Minimal/measurable residual disease (MRD) analysis has been extensively applied to follicular lymphoma (FL), which represents the main focus of this review.2,3 MRD in other iNHLs is starting to be explored, and we briefly comment on this at the end of the article.
Follicular lymphoma
FL is the second most frequent non-Hodgkin lymphoma. Despite the improvement in outcome, mainly due to the combination of anti-CD20 monoclonal antibodies with chemotherapy, most patients relapse, and the disease remains uncurable.4 The clinical course of FL is heterogeneous, with some patients not requiring treatment for years, others experiencing long-lasting remissions after first-line treatment, and ~20% rapidly relapsing within 24 months from treatment initiation.5 Transformation into an aggressive lymphoma, whose frequency has decreased with the use of rituximab (R), strongly impairs patients' survival.6 The current prognostic scores (follicular lymphoma international prognostic index [FLIPI], FLIPI-2, PRIMA-prognostic index [PRIMA-PI], follicular lymphoma evaluation index [FLEX]), based on clinical parameters, fail to predict the clinical course of individual patients.7,8 Knowledge of FL's biological heterogeneity, which relies on the complex interactions between nonmalignant immune/stromal components and tumor cells, has not identified clinically applicable predictive biomarkers.9,10
The molecular hallmark of FL, the t(14;18)(q32;q21) translocation, resulting in the hybrid BCL2/heavy chain immunoglobulin gene (IGH) rearrangement, is the first necessary but not sufficient step in lymphomagenesis.11 The BCL2/IGH gene can be used to support FL diagnosis and to evaluate treatment response in terms of MRD. The first evidence on the value of MRD in FL goes back to 1991.12 Thereafter, treatment combinations have deeply changed, as well as the techniques to measure MRD, which is currently evaluated only in the setting of clinical trials.7
Here, we discuss the current evidence on the role of MRD in the management of FL, starting from 2 clinical cases.
CLINICAL CASES
Patient 1. A 49-year-old man with FL grade 2, Ann Arbor stage IV, high-risk FLIPI, high-tumor burden and major breakpoint region (MBR)+ in PB/BM was treated in a clinical trial from July 2017 with R-bendamustine, followed by 3 courses of 4-weekly doses of R maintenance, completed in August 2019. At the end of induction (EOI), a positron emission tomography (PET)−/MRD+ response was documented. MRD remained positive throughout maintenance and at the end of treatment. In March 2021, 19 months after maintenance completion, he presented with an abdominal bulky disease recurrence. The new biopsy specimen showed FL grade 3A; the BM biopsy specimen showed no lymphoma infiltration.
Patient 2. Based on the biopsy specimen of a 3-cm inguinal lymph node, in May 2016, an asymptomatic 63-year-old woman was diagnosed with FL grade 1 to 2, Ann Arbor stage I, MBR+ in PB/BM. She received involved-site radiation (24 Gy), followed by ofatumumab consolidation for MRD+ response, as per clinical trial. She became MRD−, which persisted for 1.5 years at a 6-month MRD monitoring. In August 2018, she returned MRD+ in the BM, shortly followed by a clinical relapse.
Is molecular tumor burden at diagnosis useful to stratify patients in risk categories?
The tumor burden molecular quantification at diagnosis predicts progression-free survival (PFS) in patients with FL, in both advanced and localized stages (Table 1). Rambaldi et al13 selected patients with FL for the presence of BCL2/IGH positivity in the BM and treated them with cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP), followed by 4-weekly R in MRD+ cases, and divided them into low (43%), intermediate (34%), and high risk (23%) according to BM BCL2/IGH real-time quantitative (RQ)–polymerase chain reaction (PCR) levels at diagnosis. High BCL2/IGH+ levels were significantly associated with a reduced event-free survival (EFS) and were an independent predictor of poor clinical and molecular response in multivariate analysis (MVA). In contrast, PB BCL2/IGH levels at diagnosis were not predictive of EFS.
Studies reporting on MRD detection and monitoring in FL
| Study | Advanced disease | Patients | Therapy | Tissue | Method | Marker | Tumor burden | MRD− % | Clinical impact | Follow-up |
|---|---|---|---|---|---|---|---|---|---|---|
| Rambaldi et al13 | BCL2/IGH + FL, untreated | 128 (79 received R) | CHOP × 6 4 weeks R in PCR + patients | BM ± PB | Nested PCR | Enrolled PCR + patients (BCL2/IGH 100%) | — | End of CHOP: BM MRD− 36% (43/118) PB MRD− 35% (43/121) After R: MRD− 59 % at week 12, 74 % at week 28, and 63% at week 44 | 3-year FFR BM MRD− after CHOP 52% BM MRD− after R at week 44, 3-year FFR 57% vs 20% MRD+ | 17 months (8-39) |
| Rambaldi et al14 | BCL2/IGH + FL, untreated | 86 (same series) | BM | RQ-PCR | Enrolled PCR + patients (BCL2/IGH 100%) | At baseline: Low (1 cell in 103–105): 43 %; intermediate (1 cell in 102–103): 34 %; high (>1 cell in 102): 23 % CR: 71 % in low vs 26 % in high EFS: 59 % in low/intermediate vs 32% in high | See above | FFR: 64 % MRD− vs 32 % MRD + (P < .006) | 56 months (40-75) | |
| Ladetto et al15 | High-risk FL untreated <60 years | 134 | Phase 3 R-HDS vs CHOP × 6 + R × 4 (GITMO/IIL) | BM | Nested PCR | 73/104 (70 %) BCL2/IGH (65) + IGH (8) | — | Overall, 65 % (39/60) MRD− After CHOP-R: MRD− 44% After R-HDS: MRD− 80% (P < .002) | PFS MRD− vs MRD + (P < .001), regardless of treatment arm | 51 months |
| Bruna et al16 | High-risk FL untreated <60 years | 134 | Update of the phase 3 R-HDS vs CHOP × 6 + R × 4 (GITMO/IIL) | BM | Nested PCR | — | Overall, 65% (39/60) MRD− | 13-year OS R-HDS 64.5 % vs 68.5 % CHOP-R 13-year OS BM MRD− 82.1 % vs BM MRD + 51.9 % (P =.030) 20/24 (83 %) patients with 4-year long-term MRD− in first CR | 13 years | |
| Ladetto et al17 | FL >60 years, untreated | 227 | ML17638 R-FND × 4 + 4R ± 4R every 2 months | BM | RQ-PCR | 116/227 (BCL2/IGH 51 %) | PFS: 80 % in low vs 75 % in intermediate vs 66 % in high PFS: 61% at month + 42 in both PCR + and PCR − at baseline | At EOI: MRD− 70 % End of consolidation: MRD− 84 % | 3-year PFS: at end of consolidation: 72 % MRD− vs 39 % MRD + (16 %) (P <.007) Median PFS: 12 months MRD− (RQ-PCR); 75 % of MRD− free of PD at 36 months (P < .001) PFS maintenance arm: 83 % PCR− vs 60 % PCR + (P = .007) PFS observation arm: 71 % PCR− vs 50 % PCR + (P < .001) | 42 months |
| Galimberti et al18 | FL untreated | 415 | Phase 3 FOLL05 trial R-CHOP, R- CVP, R-FN | BM | Nested PCR; RQ-PCR | 220/415 (BCL2/IGH 53%) RQ-PCR in 105 cases | At diagnosis: 61.9% PCR+ non-CR vs 38.1% PCR− (P = .027) BM biopsy+ 32% non-CR vs 21.8% in BM− cases (P = .021) 3-year PFS: 74% in PCR−/BM− at diagnosis vs 55% in PCR+/BM+ (P = .04) ORR 38.9% in high RQ vs 76.6% in low (P = .006) Relapses: 22% in <1 × 10–4 copies vs 78% in >1 × 10–4 copies (P = .033) at baseline 3-year PFS: 80% in low vs 59% in high (P = .015) | EOI MRD− (qPCR): 109/154 (70.8%) (no difference between arms) R-CHOP 39% R-FN 36% R-CVP 25% RQ decrease >3 log: R-CHOP 42.1% R-FN 36.8% R-CVP 21.1% (P = .07) | Relapse rate: 33% for MRD− vs 41% for MRD+ at EOI (P = .363) 3-year PFS 64.3% for MRD− vs 53.1 for MRD+ at EOI (P= .08) 3-year PFS 66% for 63 MRD− vs 41% for 24 MRD+ at 12 months from EOI (P = .015) 3-year PFS 84% for 46 MRD− vs 50% for 19 MRD+ at 24 months (P = .014) | NA |
| Zohren et al19 | FL, untreated | 114 | Phase 3 NHL1-2003 trial R-CHOP vs R-B | PB | RQ-PCR | 114/173 (BCL2/IGH 66%) | Median PFS: 22 months in high BCL2/IGH (ratio >1, n = 28) vs NR in intermediate (ratio 0.1-1, n = 24) vs NR in low (<0.1, n = 55) High vs intermediate: HR, 4.28; 95% CI, 1.70-10.77 (P = .002) High vs low: HR, 3.02; 95% CI, 1.55-5.86 (P = .001) | Overall MRD− 78/92 (85%) After R-B MRD− 43/48 (89.6%) After R-CHOP MRD− 35/44 (79.5%) | 3-year PFS 63% overall | 41 months (0-69) |
| Pott et al20,21 | FL, untreated | 1101 | Phase 3 Gallium trial R vs G (CVP, B, CHOP) + maintenance | PB ± BM | RQ-PCR Nested PCR | 968/1101 (BCL2/IGH + IGH 88%) 815 (74%) suitable for RQ-PCR | Clonal marker vs no marker at baseline: stage IV 61% vs 34%; BM biopsy infiltration 58.2% vs 14.3%; high-risk FLIPI 44.5% vs 30.8%; extranodal involvement 70% vs 40% | MI PB MRD−: G-vs R-based treatment (94% vs 89%, P =.013) EOI PB ± BM MRD−: G- vs R-based treatment (92% vs 85%, P = .0041) EOI BM MRD−: G- vs R-based treatment (93% vs 83%, P =.0014), NS in the PB EOI MRD− PB ± BM: R-CVP 76% vs G-CVP 91.4%; R-CHOP 77.8% vs G-CHOP 91.3%; R-B 89.6% vs G-B 92.5% EOI PB MRD−: R-CVP 79% vs G-CVP 94%; R-CHOP 93% vs G-CHOP 96%; R-B 96% vs G-B 96% EOI BM MRD−: R-CHOP 74% vs G-CHOP 93%; R-B 87% vs G-B 93% EOI MRD+: 22/24 (92%) patients in the G-chemo arm and 36/46 (78%) patients in the R-chemo arm achieved MRD negativity early during maintenance | 4-year PFS: 80% early responders (PB MI MRD−/EOI MRD−) vs 30% PB MI MRD +/EOI MRD + (P < .0001) vs 60% late responders, PB MI MRD +/EOI MRD− (P = .0133) EOI MRD− significantly affected PFS (HR, 0.38; 95% CI, 0.26-0.56; P < .0001) and OS (HR, 0.35; 95% CI, 0.17-0.72; P = .0027) | 57 months |
| Delfau-Larue et al22 | FL untreated | 440 | Phase 3 Relevance trial R2 (18 cycles of lenalidomide plus R, followed by R maintenance therapy every 8 weeks for 12 cycles) vs R-chemo (CHOP) followed by R-maintenance every 8 weeks for 12 cycles | PB ± BM | ddPCR | 222/440 (BCL2/IGH 50.45%) BCL2/IGH+ patients: stage III-IV disease (96% vs 90%, P = .004), FLIPI score >1 (91% vs 83%, P = .002), BM involvement (62% vs 48%, P = .003) | Tumor burden 10 times higher in PB and BM of patients with week 24 MRD+, compared to patients with week 24 MRD− (P = .03 and .02) | At EOI (week 24): PB MRD− 98%, BM MRD− 78% R2 arm: MRD− 105/117; 90% vs R-chemo MRD− 70/90; 77% (P = .022) | 3-year PFS: 84% for MRD− (in PB and/or BM) vs 55% for MRD+ (P = .015) 3-year PFS: 85% for BM MRD− vs 54% for BM MRD+ (P = .011) MRD+ at EOI: R-chemo arm (HR, 3.3; 95% CI, 1.2-9.2; P = .02) vs R2 arm (HR, 2; 95% CI, 0.6-6.8; P = .27) | NA |
| Pott et al23 | R refractory FL | Phase 3 GADOLIN trial G-B + G maintenance vs B | PB ± BM | RQ-PCR (and subsequent nested) | 71% (228/319) (63% BCL2/IGH+ [MBR, mcr, 3′MBR] and 72% IGH) 52% (166/319) suitable for RQ-PCR ≤10-4 | At MI: PB MRD− 79% (41/52) in G-B vs 47% (17/36) in B (P = .0029) At EOI, PB or BM MRD− 86% (54/63) in G-B vs 55% (30/55) in B (P = .0002) | PFS (HR, 0.33; P < .0001) and OS (HR, 0.39; P = .008) for MRD− PFS in MRD +3.3 months in both arms in MRD− 8.54 B vs 35.71 G-B | 31.8 months | ||
| Study | Localized disease | Patients | Therapy | Tissue | Method | Marker | Tumor burden | MRD− % | Clinical impact | Follow-up |
| Pulsoni et al24 | Stage I (78%) Stage II (22%) untreated FL | 67 | IFRT (24-30 Gy) (+4 weeks R in MRD+ from 2005 in 19 patients) | PB ± BM | Nested PCR RQ-PCR ddPCR | 72% | 84-month PFS: 75% for BCL2/IGH- vs 59% for BCL2/IGH+ at baseline (P = .26) 84-month PFS: 90.9% in 11patients with MRD <10−5 vs 38% in 19 patients with MRD ≥10−5 by ddPCR at baseline (P = .015) | After RT: MRD −50% After R: 16/19 (84%) MRD− | Different PFS in MRD+ patients post-IFRT: between untreated patients vs patients treated with R after 2005 (P = .049) Different PFS of MRD+ patients during the follow-up vs persistently MRD− patients (P = .038) | 82 months (17-196) |
| Herfarth et al25 | Stage I (56%) Stage II (44%) untreated FL | 85 (60 long term) | MIR trial R × 8 cycles + IFRT (30-40 Gy) | 83 (64 PB, 13 BM) | Overall 24/64 (38%; PB 35%, BM 46%) Stage II > stage I (P = .0038) | 57% below 10−4 | MRD−: 20/21 (95%) at week 18 | 15/19 patients MRD− with no progression; 3 patients relapsed, in 2 associated or predicted by MRD+ sample | 29.6 months |
| Study | Advanced disease | Patients | Therapy | Tissue | Method | Marker | Tumor burden | MRD− % | Clinical impact | Follow-up |
|---|---|---|---|---|---|---|---|---|---|---|
| Rambaldi et al13 | BCL2/IGH + FL, untreated | 128 (79 received R) | CHOP × 6 4 weeks R in PCR + patients | BM ± PB | Nested PCR | Enrolled PCR + patients (BCL2/IGH 100%) | — | End of CHOP: BM MRD− 36% (43/118) PB MRD− 35% (43/121) After R: MRD− 59 % at week 12, 74 % at week 28, and 63% at week 44 | 3-year FFR BM MRD− after CHOP 52% BM MRD− after R at week 44, 3-year FFR 57% vs 20% MRD+ | 17 months (8-39) |
| Rambaldi et al14 | BCL2/IGH + FL, untreated | 86 (same series) | BM | RQ-PCR | Enrolled PCR + patients (BCL2/IGH 100%) | At baseline: Low (1 cell in 103–105): 43 %; intermediate (1 cell in 102–103): 34 %; high (>1 cell in 102): 23 % CR: 71 % in low vs 26 % in high EFS: 59 % in low/intermediate vs 32% in high | See above | FFR: 64 % MRD− vs 32 % MRD + (P < .006) | 56 months (40-75) | |
| Ladetto et al15 | High-risk FL untreated <60 years | 134 | Phase 3 R-HDS vs CHOP × 6 + R × 4 (GITMO/IIL) | BM | Nested PCR | 73/104 (70 %) BCL2/IGH (65) + IGH (8) | — | Overall, 65 % (39/60) MRD− After CHOP-R: MRD− 44% After R-HDS: MRD− 80% (P < .002) | PFS MRD− vs MRD + (P < .001), regardless of treatment arm | 51 months |
| Bruna et al16 | High-risk FL untreated <60 years | 134 | Update of the phase 3 R-HDS vs CHOP × 6 + R × 4 (GITMO/IIL) | BM | Nested PCR | — | Overall, 65% (39/60) MRD− | 13-year OS R-HDS 64.5 % vs 68.5 % CHOP-R 13-year OS BM MRD− 82.1 % vs BM MRD + 51.9 % (P =.030) 20/24 (83 %) patients with 4-year long-term MRD− in first CR | 13 years | |
| Ladetto et al17 | FL >60 years, untreated | 227 | ML17638 R-FND × 4 + 4R ± 4R every 2 months | BM | RQ-PCR | 116/227 (BCL2/IGH 51 %) | PFS: 80 % in low vs 75 % in intermediate vs 66 % in high PFS: 61% at month + 42 in both PCR + and PCR − at baseline | At EOI: MRD− 70 % End of consolidation: MRD− 84 % | 3-year PFS: at end of consolidation: 72 % MRD− vs 39 % MRD + (16 %) (P <.007) Median PFS: 12 months MRD− (RQ-PCR); 75 % of MRD− free of PD at 36 months (P < .001) PFS maintenance arm: 83 % PCR− vs 60 % PCR + (P = .007) PFS observation arm: 71 % PCR− vs 50 % PCR + (P < .001) | 42 months |
| Galimberti et al18 | FL untreated | 415 | Phase 3 FOLL05 trial R-CHOP, R- CVP, R-FN | BM | Nested PCR; RQ-PCR | 220/415 (BCL2/IGH 53%) RQ-PCR in 105 cases | At diagnosis: 61.9% PCR+ non-CR vs 38.1% PCR− (P = .027) BM biopsy+ 32% non-CR vs 21.8% in BM− cases (P = .021) 3-year PFS: 74% in PCR−/BM− at diagnosis vs 55% in PCR+/BM+ (P = .04) ORR 38.9% in high RQ vs 76.6% in low (P = .006) Relapses: 22% in <1 × 10–4 copies vs 78% in >1 × 10–4 copies (P = .033) at baseline 3-year PFS: 80% in low vs 59% in high (P = .015) | EOI MRD− (qPCR): 109/154 (70.8%) (no difference between arms) R-CHOP 39% R-FN 36% R-CVP 25% RQ decrease >3 log: R-CHOP 42.1% R-FN 36.8% R-CVP 21.1% (P = .07) | Relapse rate: 33% for MRD− vs 41% for MRD+ at EOI (P = .363) 3-year PFS 64.3% for MRD− vs 53.1 for MRD+ at EOI (P= .08) 3-year PFS 66% for 63 MRD− vs 41% for 24 MRD+ at 12 months from EOI (P = .015) 3-year PFS 84% for 46 MRD− vs 50% for 19 MRD+ at 24 months (P = .014) | NA |
| Zohren et al19 | FL, untreated | 114 | Phase 3 NHL1-2003 trial R-CHOP vs R-B | PB | RQ-PCR | 114/173 (BCL2/IGH 66%) | Median PFS: 22 months in high BCL2/IGH (ratio >1, n = 28) vs NR in intermediate (ratio 0.1-1, n = 24) vs NR in low (<0.1, n = 55) High vs intermediate: HR, 4.28; 95% CI, 1.70-10.77 (P = .002) High vs low: HR, 3.02; 95% CI, 1.55-5.86 (P = .001) | Overall MRD− 78/92 (85%) After R-B MRD− 43/48 (89.6%) After R-CHOP MRD− 35/44 (79.5%) | 3-year PFS 63% overall | 41 months (0-69) |
| Pott et al20,21 | FL, untreated | 1101 | Phase 3 Gallium trial R vs G (CVP, B, CHOP) + maintenance | PB ± BM | RQ-PCR Nested PCR | 968/1101 (BCL2/IGH + IGH 88%) 815 (74%) suitable for RQ-PCR | Clonal marker vs no marker at baseline: stage IV 61% vs 34%; BM biopsy infiltration 58.2% vs 14.3%; high-risk FLIPI 44.5% vs 30.8%; extranodal involvement 70% vs 40% | MI PB MRD−: G-vs R-based treatment (94% vs 89%, P =.013) EOI PB ± BM MRD−: G- vs R-based treatment (92% vs 85%, P = .0041) EOI BM MRD−: G- vs R-based treatment (93% vs 83%, P =.0014), NS in the PB EOI MRD− PB ± BM: R-CVP 76% vs G-CVP 91.4%; R-CHOP 77.8% vs G-CHOP 91.3%; R-B 89.6% vs G-B 92.5% EOI PB MRD−: R-CVP 79% vs G-CVP 94%; R-CHOP 93% vs G-CHOP 96%; R-B 96% vs G-B 96% EOI BM MRD−: R-CHOP 74% vs G-CHOP 93%; R-B 87% vs G-B 93% EOI MRD+: 22/24 (92%) patients in the G-chemo arm and 36/46 (78%) patients in the R-chemo arm achieved MRD negativity early during maintenance | 4-year PFS: 80% early responders (PB MI MRD−/EOI MRD−) vs 30% PB MI MRD +/EOI MRD + (P < .0001) vs 60% late responders, PB MI MRD +/EOI MRD− (P = .0133) EOI MRD− significantly affected PFS (HR, 0.38; 95% CI, 0.26-0.56; P < .0001) and OS (HR, 0.35; 95% CI, 0.17-0.72; P = .0027) | 57 months |
| Delfau-Larue et al22 | FL untreated | 440 | Phase 3 Relevance trial R2 (18 cycles of lenalidomide plus R, followed by R maintenance therapy every 8 weeks for 12 cycles) vs R-chemo (CHOP) followed by R-maintenance every 8 weeks for 12 cycles | PB ± BM | ddPCR | 222/440 (BCL2/IGH 50.45%) BCL2/IGH+ patients: stage III-IV disease (96% vs 90%, P = .004), FLIPI score >1 (91% vs 83%, P = .002), BM involvement (62% vs 48%, P = .003) | Tumor burden 10 times higher in PB and BM of patients with week 24 MRD+, compared to patients with week 24 MRD− (P = .03 and .02) | At EOI (week 24): PB MRD− 98%, BM MRD− 78% R2 arm: MRD− 105/117; 90% vs R-chemo MRD− 70/90; 77% (P = .022) | 3-year PFS: 84% for MRD− (in PB and/or BM) vs 55% for MRD+ (P = .015) 3-year PFS: 85% for BM MRD− vs 54% for BM MRD+ (P = .011) MRD+ at EOI: R-chemo arm (HR, 3.3; 95% CI, 1.2-9.2; P = .02) vs R2 arm (HR, 2; 95% CI, 0.6-6.8; P = .27) | NA |
| Pott et al23 | R refractory FL | Phase 3 GADOLIN trial G-B + G maintenance vs B | PB ± BM | RQ-PCR (and subsequent nested) | 71% (228/319) (63% BCL2/IGH+ [MBR, mcr, 3′MBR] and 72% IGH) 52% (166/319) suitable for RQ-PCR ≤10-4 | At MI: PB MRD− 79% (41/52) in G-B vs 47% (17/36) in B (P = .0029) At EOI, PB or BM MRD− 86% (54/63) in G-B vs 55% (30/55) in B (P = .0002) | PFS (HR, 0.33; P < .0001) and OS (HR, 0.39; P = .008) for MRD− PFS in MRD +3.3 months in both arms in MRD− 8.54 B vs 35.71 G-B | 31.8 months | ||
| Study | Localized disease | Patients | Therapy | Tissue | Method | Marker | Tumor burden | MRD− % | Clinical impact | Follow-up |
| Pulsoni et al24 | Stage I (78%) Stage II (22%) untreated FL | 67 | IFRT (24-30 Gy) (+4 weeks R in MRD+ from 2005 in 19 patients) | PB ± BM | Nested PCR RQ-PCR ddPCR | 72% | 84-month PFS: 75% for BCL2/IGH- vs 59% for BCL2/IGH+ at baseline (P = .26) 84-month PFS: 90.9% in 11patients with MRD <10−5 vs 38% in 19 patients with MRD ≥10−5 by ddPCR at baseline (P = .015) | After RT: MRD −50% After R: 16/19 (84%) MRD− | Different PFS in MRD+ patients post-IFRT: between untreated patients vs patients treated with R after 2005 (P = .049) Different PFS of MRD+ patients during the follow-up vs persistently MRD− patients (P = .038) | 82 months (17-196) |
| Herfarth et al25 | Stage I (56%) Stage II (44%) untreated FL | 85 (60 long term) | MIR trial R × 8 cycles + IFRT (30-40 Gy) | 83 (64 PB, 13 BM) | Overall 24/64 (38%; PB 35%, BM 46%) Stage II > stage I (P = .0038) | 57% below 10−4 | MRD−: 20/21 (95%) at week 18 | 15/19 patients MRD− with no progression; 3 patients relapsed, in 2 associated or predicted by MRD+ sample | 29.6 months |
Only trials including anti-CD20 monoclonal antibodies have been included.
FN, fludarabine and mitoxantrone; FND, fludarabine, mitoxantrone, and dexamethasone; IFRT, involved field radiotherapy; MIR, Mabthera and Involved field Radiotherapy (NCT00509184); NA, not available; NS, not significant; ORR, overall response rate; qPCR, quantitative PCR.
In large first-line trials employing R-based chemoimmunotherapy for advanced FL, BCL2/IGH was found in 51% to 66% of enrolled patients.17-19,22 Conversely, in the unpublished MRD results from the Gallium trial, in which obinutuzumab (G)–based chemotherapy plus G-maintenance resulted superior to R-chemotherapy plus R-maintenance, a clonal marker was detected in 88% of 1101 patients, higher than in other studies, because both BCL2/IGH and IGH rearrangements were screened by consensus PCR.20,21
RQ-PCR stratified patients with low, intermediate, and high BM tumor burden at diagnosis with a significantly different PFS, both in elderly patients treated within the ML17638 trial (short chemoimmunotherapy followed by a consolidation with R plus a randomized maintenance) and in the FOLL05 trial, randomly assigning patients to R-CHOP, R-fludarabine, and mitoxantrone or R-cyclophosphamide, vincristine, and prednisone (CVP).17,18 In the former, the molecular tumor burden was correlated to BM invasion but not with FLIPI.17 In the latter, high BCL2/IGH levels at enrollment, documented in patients with high FLIPI and FLIPI2 scores, were significantly associated with a lower overall response rate and a higher relapse rate and retained a negative impact on 3-year PFS besides high FLIPI and lack of complete response (CR), independently from the randomization arm.18 Likewise, in the NHL1-2003 trial, comparing R-CHOP to R-bendamustine, high pretreatment PB BLC2/IGH levels were associated with BM involvement, stage IV, high tumor burden, and increased β2-microglobulin, being an independent prognostic marker for PFS and further stratifying patients with intermediate/high FLIPI.19
In the Relevance trial, comparing the chemotherapy-free regimen lenalidomide + R (R2) vs R + chemotherapy followed by maintenance, molecular tumor burden at diagnosis quantified by droplet digital PCR (ddPCR) was significantly associated with the MRD status at week 24 (EOI).22
In early stage FL, despite a negative BM biopsy, BCL2/IGH+ cells spreading from the original lymph node could be detected in the PB/BM at diagnosis in more than 50% of patients.24,26 The 84-month PFS was 90.9% in patients with undetectable/low levels (<1 × 10−5) of circulating BCL2/IGH+ cells quantified by ddPCR at diagnosis vs 38% in those with higher levels (P = .015).24
Final comment. Both in advanced and localized FL, quantification of molecular tumor burden at baseline by RQ-PCR or ddPCR predicts PFS, being an independent prognostic marker. Circulating BCL2/IGH levels, which may simply reflect not only tumor burden but also the enhanced lymphoma cell migration and invasiveness, could help to refine our capacity to risk-stratify patients.
Is MRD useful to refine the clinical response?
In the pre-R era, several trials showed that autologous stem cell transplant induced higher rates of molecular remission (60%-70%) than standard anthracycline-based chemotherapy (30%-50%).2,3 In the R era, the addition of R induced a conversion to a MRD− status in 70% of patients MRD+ after CHOP and in 70% to 84% after R-fludarabine, mitoxantrone, and dexamethasone (FND).13,14,17 The combination of chemotherapy with R frontline showed an increased MRD− response rate at EOI compared with chemotherapy alone, with a preferential MRD clearance in the PB (Figure 1, Table 1).13-15,17-22,24,26-28 In the Gallium trial, the BM MRD− rates at EOI in the R-chemo arm were higher than previously reported and increased further in the G-arm, especially after CHOP/CVP. Indeed, G abrogated the compartment- and chemo-related effects observed in the R-arm. MRD response rates in the PB were similar across all chemo regimens (96% G-bendamustine [B], 96% G-CHOP, 94% G-CVP), as well as in the BM (93% after G-B, 93% after G-CHOP).20,21
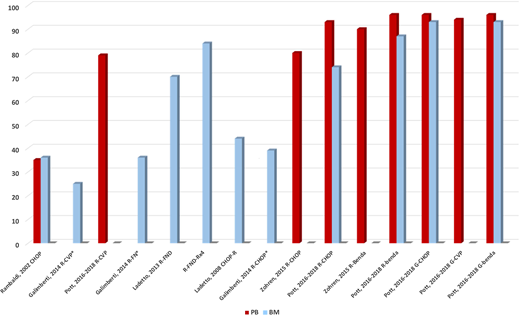
Rates of MRD negativity after anti-CD20 based treatments in advanced FL. *Data are expressed as proportion of MRD− cases at EOI. gDNA, genomic DNA.
Rates of MRD negativity after anti-CD20 based treatments in advanced FL. *Data are expressed as proportion of MRD− cases at EOI. gDNA, genomic DNA.
The importance of MRD was also shown in the Relevance trial, where MRD was quantified for the first time by ddPCR. At EOI, 98% and 78% of patients achieved a complete molecular response in the PB and BM. A complete molecular response was reached more frequently with R2 (90%) than with R-chemo (77%) (P = .022) (Figure 1, Table 1).22
In advanced stage FL, since MRD− status after treatment can be detected in patients in CR or partial response (PR), the molecular and clinical/radiologic response can be combined to refine prognosis. Ladetto et al17 showed that at month +8, 69% of patients were CR/nested PCR−, 15% PR/PCR−, and 11% CR/PCR+, with a 3-year PFS of 77%, 59%, and 45%, respectively; the 3 PR/PCR+ cases relapsed within 23 months. Similar results were shown in the FOLL05, where PFS was significantly longer in CR-PR/PCR− than in CR-PR/PCR+ patients.18 As in the Relevance study,22 the predictive value of MRD was superior to clinical response in MVA.18
Luminari et al,29 in a small subgroup of patients (n = 41) from the FOLL05 trial, suggested the complementary role of MRD and PET at EOI in defining the response to treatment, with a concordance of 76%. The 3-year PFS was 78%, 50%, and 27% in 28 PET−/MRD−, 8 PET − /MRD + , and 5 PET+ cases, respectively (P = .015). The concomitant PET/MRD negativity was associated with a better outcome: 5-year PFS 75% PET−/MRD− vs 35% PET+ or MRD+ (P = .012).29 The complementary role of PET and MRD was further supported in 298 patients from the Gallium trial: PET−/MRD+ or PET + /MRD− patients had a 2.1 higher risk of progression or death than those with both PET−/MRD−. Nevertheless, 15% of PET−/MRD− patients progressed within 2.5 years from EOI.30
Final comment. The introduction of chemoimmunotherapy with R and G has allowed an increase in the rates of MRD negativity at EOI up to 70% to 80% and 90%, respectively. MRD analysis is a sensitive tool to refine clinical response assessment in FL. In addition, the combination of molecular and metabolic response assessment is a promising and valuable tool to be further explored.
Is MRD useful to predict PFS?
The prognostic impact of MRD in advanced FL has been demonstrated across different treatment strategies. All chemoimmunotherapy trials, with or without maintenance, are associated with a significant improvement of PFS in molecular responders, independent from other prognostic factors (Table 1). Rambaldi et al13 showed that the achievement of a BM PCR− status was associated with a higher freedom-from-recurrence (FFR) (64% vs 32% for PCR+ patients). Interestingly, this study anticipated later observations17,18,21 (ie, most PCR− patients after 6 cycles were already negative after 3 cycles, and a delayed MRD clearance induced by R was possible). In the phase 3 Gruppo Italiano Trapianto Midollo Osseo/Intergruppo Italiano Linfomi (GITMO/IIL) trial, comparing high-dose sequential chemotherapy with R and autograft (R–high dose sequential chemotherapy with autografting [HDS]) to R-CHOP, molecular remission—documented in 44% of R-CHOP–treated patients and 80% of R-HDS–treated patients—was the strongest predictor of PFS, EFS, and FFR.15 The outcome of patients achieving an MRD− response was similar regardless of the treatment received, as was the outcome of patients remaining MRD+.15 In the phase 3 ML17638 trial,17 MRD negativity (by PCR and RQ-PCR) at the end of consolidation (month +8) was associated with a longer 3-year PFS, representing an independent predictor of outcome, besides clinical response and FLIPI.17 Galimberti et al18 showed that the BM MRD status at 12 and 24 months from EOI, but not at the EOI, predicted the 3-year PFS. In a MVA including FLIPI, BM involvement, quality of response, and arm of therapy, MRD persistence at month +12 (besides BM involvement) and at month +24 (alone) retained a poor prognostic role. Zohren et al19 showed that a persistent PB BCL2/IGH positivity (n = 14, 15%) after R-chemotherapy was associated with a shorter PFS (8.7 months vs not reached, P = .002), despite the 2-log reduction in BCL2/IGH levels and in both treatment arms. By MVA, both pretreatment and posttreatment BCL2/IGH levels were significant prognostic factors, the former being the strongest.
Recently, 3 studies provided the first evidence that a MRD− achievement following treatment is associated also with a prolonged OS. The long-term follow-up of a British trial showed the longer survival of MRD− responders after 2 different chemotherapy regimens in the pre-R era.31 The updated results of the phase 3 GITMO/IIL trial showed a 13-year OS of 82.1% and 51.9% for BM MRD− vs MRD+ patients.16 Moreover, in a subgroup of molecularly monitored patients for a median of 4 years since treatment completion, 20 of 24 (83%) patients alive in CR remained in first MRD− response, raising the hypothesis of a functional cure also for FL. In the Gallium trial, at an updated median follow-up of 57 months, MRD− patients at EOI (n = 564) had a longer PFS than MRD+ (n = 70) (P < .0001) and a better OS (P = .0027).21
The Gallium trial also opened the way to novel concepts.21 (i) The role of maintenance either maintained or increased MRD− response rates. Indeed, two-thirds of MRD− responses were preserved throughout maintenance (G, 67.0%; R, 63.2%) with no difference between the 2 arms in the rate of conversion to MRD+ (6.3% vs 6.1%, respectively). Furthermore, within MRD+ patients at EOI, 92% of 24 patients in the G-chemo and 78% of 46 in the R-chemo arm became MRD− in the first months of maintenance; the few cases who were never MRD− rapidly progressed. (ii) For the first time, MRD was assessed not only at EOI but also at the middle of induction (MI). PFS was significantly longer for PB MRD− vs MRD+ at MI (P < .0001), with early responders (MI MRD−/EOI MRD−) having the best prognosis.
In the Relevance trial, MRD− or MRD+ patients in the PB and/or BM at EOI had a 3-year PFS of 84% and 55%, respectively, being significant only in the BM and in the R-chemo but not in the R2 arm.22
Even in the relapse/refractory setting, the GADOLIN trial showed that MI MRD in the PB and/or BM was significantly different between the G-B and the B arm. In MVA, MRD status at EOI (85.7% G-B vs 55% B-arm), treatment arm and FLIPI status were strongly predictive of PFS and, to a lesser extent, of OS.23
In localized FL, a monocentric experience demonstrated that after treatment with local 24 to 30 Gy radiotherapy (RT), disappearance of circulating BCL2/IGH+ cells in the PB and/or BM occurred in 50% (n = 20/40) of patients.24 Additional treatment with R in MRD+ patients after RT or who had molecularly relapsed during the follow-up achieved a molecular CR in 84% of cases: the 82-month PFS of MRD+ R-treated patients was significantly better than historical controls, and the relapse probability was significantly lower in MRD− patients after RT or after R than that of patients remaining MRD+.24
Final comment. MRD negativity is predictive of a better PFS in all clinical trials conducted in the past 2 decades, even in relapsed patients, and possibly of a longer survival in studies with a prolonged follow-up. Assessment of MRD at earlier time points with respect to EOI can also be informative.
Is the prolonged molecular follow-up of clinical relevance?
The prognostic value of sequential BCL2/IGH assessment to predict clinical relapse is supported by limited evidences and often hampered by the lack of adherence to long-term MRD evaluations.18,19,21,27 In FOLL05, molecular recurrence preceded clinical relapse by a median of 5 months in 9 of 10 evaluable cases.18 Zohren et al19 over a 41-month follow-up showed that 49 patients remained BCL2/IGH– and 43 converted to BCL2/IGH+. Qualitative molecular relapse was not indicative of an inferior PFS, unless associated with high BCL2/IGH levels. In 20 patients who were rigorously sampled, the interval from BCL2/IGH redetection to clinical relapse was 9.5 months. In the Gallium trial, patients failing to become MRD− had a high likelihood of experiencing early progression or death.21
More relevant than the MRD punctual evaluation is the kinetic analysis of molecular results over time. So far, few data are available in FL. The first evidence came from Ladetto et al,17 who showed that the accumulation of MRD− results over time reduced the likelihood of relapse. Kinetic models of MRD analysis in FL are awaited.
Final comment. Patients with FL with a higher relapse probability can be identified, but the timing of clinical relapse is not accurately predicted by the current MRD analyses. Accumulating evidence suggests that a kinetic model of MRD analysis, more than a single result, could help in anticipating disease recurrence.
Can we use MRD to modulate treatment?
The first attempts to use MRD as a tool to guide therapeutic choices were provided in advanced FL, where R could convert MRD+ after CHOP to MRD−, and in localized FL after RT.13,24 Two recent large prospective Italian Fondazione Italiana Linfomi (FIL) trials explored the use of MRD to modulate treatment in FL.32,33 FOLL12 was a phase 3 trial designed to prove the feasibility of a postinduction modulation of the standard 2-year R maintenance according to metabolic response (Deauville score 1-3) and MRD response at EOI after chemoimmunotherapy in advanced FL. In the experimental arm, PET−/MRD− patients (29%) underwent observation, PET−/MRD+ patients (4%) received repeated weekly R, and PET+ patients had 1 dose of ibritumomab tiuxetan followed by standard R maintenance. The experimental arm showed a significantly inferior PFS compared with the standard 2-year R maintenance, particularly for PET−/MRD− patients.32 It appears that a single molecular response evaluation at EOI is probably not sufficient to indicate disease eradication and to deintensify treatment. Results of MRD monitoring will be shown at this meeting by Ladetto et al (Abstract submission #146773).
The MIRO' (Molecularly Immuno-Radio-therapy Oriented, EUDRACT 2012-001676-11) trial for localized FL used MRD to guide post-RT treatment.33 Thirty percent of patients had circulating BCL2/IGH+ cells,25,33 18 MRD+ patients after RT (60%) and 8 MRD+ during follow-up received ofatumumab. With this strategy, 91.7% of patients achieved a molecular CR, with a suggested clinical benefit after 38 months of follow-up.
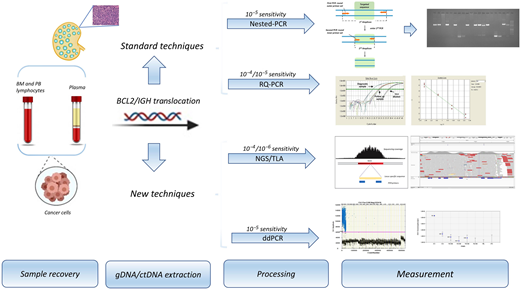
The main limitation in the introduction of MRD monitoring in the management of patients with FL, especially if considering only the BCL2/IGH rearrangement, is represented by the lack of a molecular target in a notable proportion of cases. It is hoped that technical advancements currently under investigation will overcome these limitations (Figure 2, Tables 2-3).34,35-43
Principles of standard and next-generation technologies in MRD monitoring
| Technology | References | Potential advantages and open issues |
|---|---|---|
| RQ-PCR | 1,35 | The most validated and standardized quantitative method for MRD detection in FL. Despite remarkable sensitivity and specificity, RQ-PCR has notable limitations due to the lack of BCL2/IGH target in about 40% of advanced FL and 65% to 70% of localized FL, currently not eligible for MRD assessment, and to the challenge of very low MRD levels, where it is difficult to dissect if the signal observed by PCR (not quantifiable) is due to few residual leukemic cells or to a nonspecific amplification of normal DNA. |
| NGS | 34,36 | Potential deeper sensitivity compared with the classic methods. A sensitivity of 10−6 is achievable only when high amounts of DNA are used. Broad spectrum of identifiable molecular targets: a “capture-based” protocol covering the coding V, D, J genes of the IGH loci was capable of detecting clonal rearrangements in 87% (21/24) of lymphoproliferative disorders. |
| TLA | 37,38 | Alternative NGS tool capable of sequencing structural variants, usually not detected by conventional PCR approaches, thanks to the selective amplification and sequencing of entire genes on the basis of the cross-linking of physically proximal DNA loci. |
| ddPCR | 39,40 | A third-generation quantitative method based on the partition of the template DNA into water-in-oil droplets in which PCR amplification occurs, allowing the quantification of nucleic acid targets without the need of the calibration curve. Sensitivity, accuracy, and reproducibility at least comparable to that of RQ-PCR. A good performance in the MRD quantification in at least 20% to 30% of samples resulting positive but not quantifiable by RQ-PCR. |
| cfDNA | 41-43 | Plasma is a potentially important source of DNA (ie, cfDNA), potentially useful to identify distinct biological subtypes of lymphomas and to provide insights into the patterns of genomic evolution/resistance throughout treatment in all compartments, not only PB and BM. A noninvasive tool to monitor MRD in non-Hodgkin lymphoma through patient-specific IGH rearrangements, to identify individuals at an increased risk of relapse and to detect relapse before clinical evidence of disease. Most cfDNA originates from leukocytes, and only a small fraction (<10%) is tumor derived, known as ctDNA. ctDNA concentration varies among patients and differs according to the type, location, and stage of cancer, with some producing extremely low concentrations. Thus, it is unlikely that cfDNA will reach the sensitivity of MRD analysis on circulating cells in FL. Before broad clinical implementation, issues on preanalytical factors must be addressed in order to achieve consistent and reproducible results. |
| Technology | References | Potential advantages and open issues |
|---|---|---|
| RQ-PCR | 1,35 | The most validated and standardized quantitative method for MRD detection in FL. Despite remarkable sensitivity and specificity, RQ-PCR has notable limitations due to the lack of BCL2/IGH target in about 40% of advanced FL and 65% to 70% of localized FL, currently not eligible for MRD assessment, and to the challenge of very low MRD levels, where it is difficult to dissect if the signal observed by PCR (not quantifiable) is due to few residual leukemic cells or to a nonspecific amplification of normal DNA. |
| NGS | 34,36 | Potential deeper sensitivity compared with the classic methods. A sensitivity of 10−6 is achievable only when high amounts of DNA are used. Broad spectrum of identifiable molecular targets: a “capture-based” protocol covering the coding V, D, J genes of the IGH loci was capable of detecting clonal rearrangements in 87% (21/24) of lymphoproliferative disorders. |
| TLA | 37,38 | Alternative NGS tool capable of sequencing structural variants, usually not detected by conventional PCR approaches, thanks to the selective amplification and sequencing of entire genes on the basis of the cross-linking of physically proximal DNA loci. |
| ddPCR | 39,40 | A third-generation quantitative method based on the partition of the template DNA into water-in-oil droplets in which PCR amplification occurs, allowing the quantification of nucleic acid targets without the need of the calibration curve. Sensitivity, accuracy, and reproducibility at least comparable to that of RQ-PCR. A good performance in the MRD quantification in at least 20% to 30% of samples resulting positive but not quantifiable by RQ-PCR. |
| cfDNA | 41-43 | Plasma is a potentially important source of DNA (ie, cfDNA), potentially useful to identify distinct biological subtypes of lymphomas and to provide insights into the patterns of genomic evolution/resistance throughout treatment in all compartments, not only PB and BM. A noninvasive tool to monitor MRD in non-Hodgkin lymphoma through patient-specific IGH rearrangements, to identify individuals at an increased risk of relapse and to detect relapse before clinical evidence of disease. Most cfDNA originates from leukocytes, and only a small fraction (<10%) is tumor derived, known as ctDNA. ctDNA concentration varies among patients and differs according to the type, location, and stage of cancer, with some producing extremely low concentrations. Thus, it is unlikely that cfDNA will reach the sensitivity of MRD analysis on circulating cells in FL. Before broad clinical implementation, issues on preanalytical factors must be addressed in order to achieve consistent and reproducible results. |
A major standardization effort is under way within the EuroClonality (https://www.euroclonalityngs.org/usr/pub/pub.php) and EuroMRD Consortium (www.euromrd.org), to establish guidelines for NGS and ddPCR MRD analysis and their future application in standard clinical practice.
cfDNA, cell-free DNA; NGS, next-generation sequencing; TLA, target locus amplification.
First applications of next-generation technologies to molecular monitoring in FL
| Study | Patients | Marker/tissue/timing | Method | Potential impact |
|---|---|---|---|---|
| Genuardi et al38 | 20 FL with no MBR or mcr | BCL2/TLA BM At diagnosis and for MRD | TLA | BCL2/TLA in 8 (40%) of “marker-negative” cases The new BCL2/TLA markers were suitable for RQ-PCR MRD analysis in 4 of 5 cases. MRD by BCL2-TLA reached good sensitivity levels. |
| Cavalli et al40 | 67 early stage FL | BCL2/IGH PB, BM At diagnosis and for MRD | ddPCR | Concordance between ddPCR and RQ-PCR: 82% ddPCR identified a MBR marker in 8 of 18 (44%) samples that resulted in MBR−/mcr− by qualitative nested PCR. Molecular tumor burden at diagnosis ≥10−5 significantly predicted PFS only when quantified by ddPCR but not by RQ-PCR. Higher sensitivity of ddPCR in RQ-PCR PNQ samples. |
| Sarkozy et al42 | 34 FL from PRIMA trial | IGH Tumor biopsy Plasma At diagnosis | NGS | 29 (85%) had 1 or more tumor clonotypes in the tumor biopsy specimen. 25 (74%) had 1 or more tumor clonotypes in plasma. 18 of 24 (75%) patients with an IGH clonotype had several detectable subclones in the tumor or in the plasma. 13 of 24 (54%) showed a subclone detected in both the plasma and the tumor. >50% of cases showed a different distribution of subclones between tumor and plasma. High ctDNA levels at diagnosis predicted short PFS in MVA. |
| Delfau-Larue et al43 | FL | PET TMTV (n = 133) BCL2/IGH PB CTC (n = 68) PB cfDNA (n = 61) At diagnosis | ddPCR | 23 of 68 cfDNA were BCL2/IGH+ (ctDNA ≤10% cfDNA). High correlation between CTCs and TMTV and between cfDNA and TMTV CTCs predictive of outcome in univariate analysis but not in MVA Total cfDNA levels and TMTM are independent predictors of outcome. |
| Study | Patients | Marker/tissue/timing | Method | Potential impact |
|---|---|---|---|---|
| Genuardi et al38 | 20 FL with no MBR or mcr | BCL2/TLA BM At diagnosis and for MRD | TLA | BCL2/TLA in 8 (40%) of “marker-negative” cases The new BCL2/TLA markers were suitable for RQ-PCR MRD analysis in 4 of 5 cases. MRD by BCL2-TLA reached good sensitivity levels. |
| Cavalli et al40 | 67 early stage FL | BCL2/IGH PB, BM At diagnosis and for MRD | ddPCR | Concordance between ddPCR and RQ-PCR: 82% ddPCR identified a MBR marker in 8 of 18 (44%) samples that resulted in MBR−/mcr− by qualitative nested PCR. Molecular tumor burden at diagnosis ≥10−5 significantly predicted PFS only when quantified by ddPCR but not by RQ-PCR. Higher sensitivity of ddPCR in RQ-PCR PNQ samples. |
| Sarkozy et al42 | 34 FL from PRIMA trial | IGH Tumor biopsy Plasma At diagnosis | NGS | 29 (85%) had 1 or more tumor clonotypes in the tumor biopsy specimen. 25 (74%) had 1 or more tumor clonotypes in plasma. 18 of 24 (75%) patients with an IGH clonotype had several detectable subclones in the tumor or in the plasma. 13 of 24 (54%) showed a subclone detected in both the plasma and the tumor. >50% of cases showed a different distribution of subclones between tumor and plasma. High ctDNA levels at diagnosis predicted short PFS in MVA. |
| Delfau-Larue et al43 | FL | PET TMTV (n = 133) BCL2/IGH PB CTC (n = 68) PB cfDNA (n = 61) At diagnosis | ddPCR | 23 of 68 cfDNA were BCL2/IGH+ (ctDNA ≤10% cfDNA). High correlation between CTCs and TMTV and between cfDNA and TMTV CTCs predictive of outcome in univariate analysis but not in MVA Total cfDNA levels and TMTM are independent predictors of outcome. |
CTC, circulating tumor cell; PNQ, positive not quantifiable; TMTV, total metabolic tumor volume.
Final comment. R maintenance holds and increases the rates of MRD negativity. Two recent trials (FOLL12 and MIRO') explored MRD-driven modulation of the postinduction therapy in FL, with treatment intensification or deintensification in MRD+ and MRD− patients at the EOI, respectively. Final results are awaited.
CLINICAL CASES (continued)
Patient 1. The persistence of MRD positivity during the 2-year treatment despite a PET negativity suggests a resistance to R-bendamustine treatment. Indeed, the patient quickly relapsed. In such patients, a possible intensification/switch of treatment could be explored in clinical trials.
Patient 2. Although in this localized FL, clinical relapse was anticipated by a molecular conversion to MRD positivity, this is not always the case with the current MRD monitoring timing and modalities. The clinical benefit of adding an anti-CD20 monoclonal antibody to RT in localized FL or to treat molecular relapses needs to be addressed in well-designed clinical trials.
Other iNHLs: lymphoplasmacytic lymphoma/Waldenström macroglobulinemia and marginal zone lymphoma
Although the role of MRD monitoring in FL is progressively increasing, MRD in other iNHLs, such as lymphoplasmacytic lymphoma/Waldenström macroglobulinemia (WM) and marginal zone lymphoma, is only recently starting to be explored.44,45 In WM, MYD88L265P is a diagnostic and predictive biomarker of therapy response. Besides allele-specific RQ-PCR, ddPCR has recently proved to be a suitable and sensitive tool for MYD88L265P screening and MRD monitoring.44 Both unsorted BM and PB samples can be reliably tested, as well as circulating tumor DNA (ctDNA), which represents an attractive and less invasive alternative to BM for MYD88L265P detection.44 MYD88L265P detection in the cerebral spinal fluid by ddPCR is also useful to diagnose Bing-Neel syndrome.46
Promising results have been preliminarily shown in splenic marginal zone lymphoma, where MRD has been assessed in BM and PB by ddPCR using IGH allele-specific oligonucleotide primers in the phase 2 BRISMA/IELSG36 (Bendamustine-rituximab as first-line treatment of splenic marginal zone lymphoma/International Extranodal Lymphoma Study Group) trial.45
Concluding remarks
Despite several decades of research, MRD analysis in FL has not yet entered the day-to-day clinical practice. Indeed, outside of clinical trials, MRD results should not be used to take clinical decisions in the real-life management of patients with FL. The issue of BCL2/IGH+ nonmalignant B cells that can be found in the PB of healthy individuals47 is marginal in treated patients with FL, because the emergence of a BCL2/IGH clone unrelated to the disease is very unlikely and rarely requires the need of proving the sequence identity of the rearrangement.
To move MRD in FL from clinical trials to daily practice, further studies are needed to overcome the limit represented by the lack of a molecular marker for all patients; to establish an integrated risk stratification; to demonstrate whether MRD analysis can be integrated with PET for a refined definition of “poor responders,” candidates to experimental approaches; to explore other MRD-adapted treatment modalities, possibly with kinetic models of MRD analysis; and to evaluate if chemo-free combinations have an advantage in terms of MRD achievement compared with chemoimmunotherapy. Results from new-generation clinical trials (eg, FIL FOLL12 and Gallium) are eagerly awaited. Data are mature to design MRD-driven clinical trials that incorporate the molecular monitoring in the management of patients with FL.
Acknowledgments
Work partly supported by Associazione Italiana per la Ricerca sul Cancro (AIRC), Metastases 5 x 1000 Special Program, N° 21198, Milan, Italy (Robin Foà). The authors thank Dr. Marco Ladetto and the FIL MRD network.
Conflict-of-interest disclosure
Ilaria Del Giudice: AstraZeneca, Tolero (advisory board).
Irene Della Starza: no conflicts to disclose.
Robin Foà: honoraria from Janssen, Amgen, Novartis, Incyte, Servier, and Sanofi.
Off-label drug use
Ilaria Del Giudice: nothing to disclose.
Irene Della Starza: nothing to disclose.
Robin Foà: nothing to disclose.
