

Abstract
The efficacy and tolerability of the combination of hypomethylating agents with venetoclax (HMA-VEN) in patients with newly diagnosed acute myeloid leukemia has been a practice-changing milestone in the field. However, treatment failure and relapse remain major barriers to prolonged survival. TP53 mutation is a predictor of primary induction failure and portends especially poor outcomes. Prelinical data suggest that VEN resistance stems from these genetic changes, which lead to increases in antiapoptotic proteins such as MCL-1 and BCLXL. For patients who discontinue HMA-VEN for reasons other than disease progression, such as post allotransplantation, infection, and personal preference, rechallenge with HMA-VEN at the time of relapse may be considered. For those who progress on HMA-VEN, clinical trials with novel agents or rational drug combinations are preferred if available. If no trial option is available, fit patients may benefit from intensive chemotherapy. Emerging therapies aim to overcome venetoclax resistance, target interactions that promote leukemogenesis, and harness the immune system to irradicate leukemic blasts and stem cells.
Learning Objectives
Review factors predictive of failure following HMA-VEN in patients with previously untreated AML
Identify mechanisms of venetoclax resistance in AML
Discuss treatment recommendations for patients with AML who progress after HMA-VEN chemotherapy
Review novel therapies in development for patients with relapsed or refractory AML following HMA-VEN chemotherapy
CLINICAL CASE 1
A 78-year-old man with a past medical history of hypertension and diabetes was diagnosed with acute myeloid leukemia (AML) 6 months ago. His initial bone marrow biopsy confirmed 70% myeloblasts, cytogenetics were normal, and next-generation sequencing (NGS) detected DNMT3A (variant allele frequency [VAF], 11%), NRAS (6%), and NPM1 (23%) mutations. The patient was started on azacitidine at 75 mg/m2/d on days 1 through 7 every 28 days and VEN at 400 mg/d on days 1 through 28 and achieved a complete remission (CR) with measurable residual disease (MRD) detectable by multiparametric flow cytometry after 1 cycle. He tolerated this regimen well, had a full count recovery, and remained on schedule with treatment until cycle 3, when he developed bacteremia requiring a weeklong hospitalization. Chemotherapy was withheld for 3 weeks due to illness and cytopenia. His absolute neutrophil count, 0.7 × 103/uL, while adequate, never fully recovered. Given the prolonged neutropenia, venetoclax (VEN) administration was shortened to days 1 through 14 every 28 days for the next 2 cycles. Unfortunately, he was found to have circulating peripheral blasts, which prompted a repeat bone marrow biopsy that confirmed morphologic relapse. In addition to the mutations present at diagnosis, there was a new mutation, FLT3-ITD.
Hypomethylating agents and VEN failure
Treatment options for older patients with newly diagnosed AML ineligible for intensive chemotherapy (IC) were limited until recent years, when several novel and targeted agents were introduced, perhaps none more paradigm shifting than the combination of hypomethylating agents (HMAs) with VEN. This regimen was found to significantly prolong survival when compared to azacitidine alone in the VIALE-A trial, leading to the US Food and Drug Administration's approval of frontline HMA-VEN in patients aged 75 years or older or unfit for intensive induction chemotherapy.1 Despite improved outcomes with a median duration of remission at 22 months in long-term follow-up, most patients will eventually relapse.2
Certain molecular patterns appear to predict response and treatment failures to HMA-VEN.3 An analysis of patients enrolled on the VIALE-A (HMA-VEN) and VIALE-C (low-dose cytarabine [LDAC]-VEN) clinical trials (n = 81) reported high rates of CR/CR with incomplete hematologic recovery (CRi) (>80%) in those with NPM1, IDH1/2, or DNMT3A mutations.3 The NPM1 and IDH2 subsets also demonstrated a long duration of response (DoR) from over 20 to almost 50 months.3 In contrast, patients with TP53 have a CR/CRi of 55.3% and a shorter DoR for those who do respond.1 Interestingly, clonal selection for TP53 while receiving treatment with HMA-VEN and clonal expansion that increases kinase activation were shown to contribute to the adaptive resistance observed.3 The median time to relapse for patients with adaptive resistance was 6.4 months.3
Another important prognostic biomarker is MRD.4 Of the 164 CR/CRi patients evaluable for MRD in the VIALE-A trial, 67 (41%) had undetectable MRD, defined as residual blasts of less than 0.1% by multiparametric flow cytometry.5 In patients with undetectable MRD, 25% achieved MRD negativity at the end of cycle 1, 27% at the end of cycle 4 (cumulatively 52%), 27% at the end of cycle 7 (cumulatively 79%), and 21% after cycle 7 (cumulatively 100%). This suggests that early and late responses are possible. Among patients with IDH1/2, 49% (21/43) achieved undetectable MRD and had a more favorable DoR, event-free survival, and overall survival (OS) compared to those with MRD. Notably, patients who achieved undetectable MRD at any time point had a higher incidence of NPM1 mutations at diagnosis (36% vs 3% in detectable MRD).5 Additionally, those without MRD had better outcomes according to DoR, event-free survival, and OS, with the 12-month estimates being 81.2%, 83.2%, and 94%, respectively. Upon long-term follow-up, the median OS reached 34.2 months in patients without MRD vs 18.7 months in those with detectable MRD.2
Mechanism of VEN resistance
VEN is an inhibitor of B-cell lymphoma 2 (BCL2), which is an important cellular protein that modulates intrinsic apoptosis.6 Normally, antiapoptotic proteins (BCLXL, BCL2A2, MCL-1, BCL-W, and BFL−1/A1) sequester proapoptotic proteins (eg, sensitizers and activators) via BH3 domain interactions. Sensitizers (BAD, BIK, HRK, and NOXA) and BH3 mimickers such as VEN promote apoptosis by binding to antiapoptotic proteins, thereby releasing activators (BIM, BID, and PUMA) to interact with effectors (BAK and BAX), increasing mitochondrial outer membrane permeabilization and cytochrome c–mediated cell death.7 VEN is selective for BCL2, with much lower affinity toward other family members such as BCLXL.8 VEN resistance occurs when displaced BH3-only activator proteins, instead of interacting with BAK/BAX to cause apoptosis, are sequestered by the upregulation of other BCL2 family members including BCLXL, MCL-1, and BCL2A1 (Figure 1).6 In preclinical studies, this shift of less BCL2 dependency and more BCLXL and MCL-1 expression was observed in AML cells with prolonged exposure to VEN.9
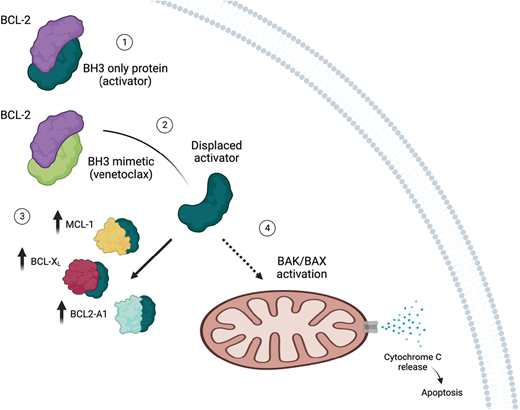
Mechanism of VEN resistance. (1) The proapoptotic BH3-only protein binds to antiapoptotic protein BCL2. (2) VEN is a BH3 mimetic that binds to BCL2, which leads to displacement of BH3-only protein. (3) In the setting of VEN resistance, increased levels of antiapoptotic proteins such as MCL-1, BCLXL, and BCL2A1 sequester BH3-only proteins. (4) Consequently, there are fewer BH3-only proteins available to induce apoptosis. Created with BioRender.com.
Mechanism of VEN resistance. (1) The proapoptotic BH3-only protein binds to antiapoptotic protein BCL2. (2) VEN is a BH3 mimetic that binds to BCL2, which leads to displacement of BH3-only protein. (3) In the setting of VEN resistance, increased levels of antiapoptotic proteins such as MCL-1, BCLXL, and BCL2A1 sequester BH3-only proteins. (4) Consequently, there are fewer BH3-only proteins available to induce apoptosis. Created with BioRender.com.
Specific somatic mutations such as those associated with cell signaling, FLT3-ITD, PTPN11, KRAS, and tumor suppression, TP53, have been shown to confer VEN resistance.10-12 FLT3-ITD mutation increases the level of BCLXL and MCL-1 via activation of the STAT5, PI3K/AKT, and RAS/MAPK signaling pathways.11 Specifically, AKT and ERK, downstream of PI3K and RAS, respectively, inhibit glycogen synthase kinase 3, resulting in decreased MCL-1 degradation.6 STAT5 regulates BCLXL gene expression and also increases MCL-1 indirectly via phosphorylation of AKT. Similarly, PTPN11 mutation upregulates BCLXL and MCL-1.10 In KRAS- mutated AML, there is upregulation of MCL-1 and BCL2A1 and downregulation of BCL2 and BAX. Based on clustered regularly interspaced short palindromic repeats/Cas9 screening and preclinical studies, TP53 knockout cells were found to have a lower level of activator and effector proteins, contributing to VEN resistance in TP53-mutated AML.12
Several studies have reported that the monocytic differentiation of blasts is a predictor of resistance to VEN-based therapy.13,14 Ex vivo drug testing of blast populations has observed high sensitivity to VEN in AML M0 and M1 but resistance to BCL2 inhibition in M4 and M5 subtypes.13 A separate study corroborated this finding and additionally suggested that azacitidine (AZA)-VEN resistance arose from intrinsic biological properties of monocytic AML cells.14 However, investigators have recently shown that clinical response to AZA-VEN is independent of myeloid differentiation.15 Rather, it is the disease-driving leukemic stem cells, whose characteristics are mainly based on mutations rather than blast differentiation state, that determine the response to AZA-VEN. Indeed, the expression of BCL2 family proteins including BCL2, BCLxL, and MCL-1 within leukemic stem cell–like cells calculated as a combinatorial score was shown to accurately predict AZA-VEN response.15
Treatment options after HMA-VEN discontinuation/failure
In patients with newly diagnosed AML who achieve a clinical response with HMA-VEN but relapse after therapy interruption or discontinuation, rechallenge is an option. In a cohort of 15 patients where reasons for stopping HMA-VEN included allogeneic hematopoietic cell transplantation (alloHCT) and invasive fungal infections where over 50% had adverse-risk disease at diagnosis, retreatment with HMA-VEN resulted in CR/CRi in 5 patients (33%), with 2 of the responders achieving MRD negativity.16 While the responses were short-lived, 1 patient was able to bridge to a second alloHCT. The median latency between initial treatment and retreatment was 224 days (range, 73-407 days).16 In a study utilizing data from the VIALE-A/C trials, 13 patients who electively discontinued treatment were identified.17 These patients were in first CR/CRi and had received at least 12 months of therapy. A total of 6 patients relapsed (67% showed molecular evolution), and 3 were retreated with the same regimen, with 2 out of 3 (66%) successfully recapturing CR/CRi.17
Despite these data, once patients progress through HMA-VEN, the overall outcome is poor. Median OS was 2 to 3 months in a retrospective study evaluating outcomes of 2 clinical trials.18 Of 95 patients, 41 (43%) had relapsed or refractory (R/R) disease to frontline HMA-VEN. Twenty-four patients received salvage therapy and only 5 responded (2 received HMA-FLT3 inhibitor, 1 received cladribine-idarubicin-cytarabine, 1 received cladribine-idarubicin-cytarabine-gemtuzumab ozogamicin, and 1 received HMA-nivolumab-ipilimumab).18 Consistent with prior reports, all patients had aggressive disease biology at diagnosis with complex cytogenetics, TP53, FLT3, and/or K/NRAS mutations.3 In a similar study but using real-world data (n = 103), 71 patients (28 relapsed, 43 refractory) were identified as R/R to frontline HMA-VEN.19 Further treatment was pursued in 11 patients, mostly in the form of targeted therapy, and CR was achieved in 3 patients. Multivariable analysis revealed that the presence of K/NRAS, TP53, and refractoriness to HMA-VEN were predictors of inferior survival.19
CLINICAL CASE 1 (continued)
This patient had a disruption of HMA-VEN due to infection and resumed therapy at a modified dose due to continued neutropenia. The patient relapsed with evidence of clonal evolution including an actionable mutation. While rechallenge with HMA-VEN at the full dose is a possibility, the likelihood of response is low. Retreatment, if chosen, should be limited to no more than 1 additional cycle with repeat bone marrow biopsy afterward to assess disease status. If no significant improvement is seen, it is unlikely that further HMA-VEN will be beneficial. Targeted therapy, specifically gilteritinib, is an option. However, if available, clinical trials using novel agents or a combination of agents including an FLT3 inhibitor should be prioritized.
CLINICAL CASE 2
A 56-year-old previously healthy woman presented to the emergency room with several weeks of worsening fatigue and easy bruising. Laboratory studies were notable for pancytopenia with circulating blasts. Bone marrow biopsy and ancillary testing revealed a 25% myeloblast marrow infiltration, complex cytogenetics, and a monoallelic TP53 (VAF, 30%) mutation (the only mutation) consistent with AML. The patient received azacitidine on days 1 through 7 every 28 days per cycle with VEN at 400 mg/d and achieved CR with undetectable MRD by flow cytometry but detectable TP53 on NGS. Unfortunately, while waiting for alloHCT, she developed a morphologic relapse and a rising TP53 VAF on NGS. Her performance status remains robust.
HMA and VEN in fit patients with adverse-risk AML
Although HMA-VEN is approved for patients who are not IC candidates, there are more patients receiving HMA-VEN who would otherwise be considered fit for IC. In a retrospective study comparing newly diagnosed AML patients treated with HMA-VEN (n = 143) or IC (n = 149), the response rates were not significantly different at 76.9% and 70.5%, respectively (P = .2109).20 Median OS was superior in the IC arm (29 vs 16 months in HMA-VEN; P = .002). However, in a propensity-matched cohort accounting for age, European LeukemiaNet risk, and alloHCT status, median OS for IC became 24 months and was not reached for HMA-VEN, with a trend toward significance (P = .0667).20 Further analysis showed that adverse risk, RUNX1 mutation, and older age were predictors of better outcomes with HMA-VEN. In a multivariate analysis, alloHCT was found to be the sole positive predictor of OS, underscoring the importance of considering this treatment modality for patients treated with either regimen. These findings provide the rationale for the ongoing clinical trial (NCT03573024) evaluating frontline HMA-VEN therapy for younger patients (aged 18-59) eligible for IC but with adverse-risk disease by European LeukemiaNet guidelines.21
Another study retrospectively evaluated the outcomes of using HMA-VEN (n = 488) or 7 plus 3 (cytarabine and anthracycline; n = 312) in newly diagnosed AML patients who were older (60-75 years) and fit.22 The median OS was 10 and 22 months for HMA-VEN and 7 plus 3, respectively (P < .0005). No subset with improved OS was identified in either regimen. Notably, in a sensitivity analysis in which only patients with a 30% to 70% chance of receiving either treatment were included (HMA-VEN: n = 120 and 7 plus 3: n = 135), the median OS was not significantly different, close to 17.5 months for both cohorts.22 This suggests that select older patients can substantially benefit from IC, while many do not. In a related study, the same authors assessed the real-world effectiveness of HMA-VEN (n = 439) and CPX-351 (n = 217) in older patients with newly diagnosed AML.23 Interestingly, the median OS for HMA-VEN (11 months) and CPX-351 (13 months) did not significantly differ (P = .22). This is despite multiple sensitivity analyses and controlling for various variables.23 A randomized clinical trial to address this question of HMA-VEN vs IC for frontline AML is ongoing (NCT04801797).
In patients with R/R disease after frontline HMA-VEN, IC as a second-line therapy is often an approach chosen for select patients. In a study of 208 newly diagnosed AML patients who received frontline HMA-VEN, 19 were relapsed (n = 6) or refractory (n = 13) and subsequently received 7 plus 3 or another cytarabine-based IC regimen.24 The response rate in this subset was 57.9% (11/19), and 81.8% (9/11) of responders proceeded to alloHCT.24 The majority had adverse-risk disease (15/19, 78.9%), as expected. Of note, these were patients treated in the second- line setting. If a patient has progressed through multiple lines of therapy, including salvage with a VEN-based regimen, the outcome is dismal. One study examined this population (n = 28), and among those who received further therapy (n = 22), only 18% had a CR.25 Treatment using IDH/FLT3 inhibitors (enasidenib, sorafenib, and gilteritinib) in 6 patients, decitabine-VEN in 5 patients, and LDAC-glasdegib in 10 patients did not yield an objective response. However, 3 out of 6 patients achieved CR with VEN-actinomycin D plus or minus LDAC despite previous VEN exposure, suggesting some patients may benefit from VEN with intensification of chemotherapy. However, the number of patients treated with this regimen is small, and results should be interpreted cautiously.25 A treatment algorithm for patients who progress after HMA-VEN is shown in Figure 2.

Treatment algorithm after HMA-VEN failure. *Combining intensive chemotherapy with a targeted agent represents an area of active research, and this treatment approach is being used off-label. **More studies are needed to assess whether adding VEN to IC can improve outcomes in the setting of post-HMA-VEN failure. BSC, best supportive care; PD, progressive disease. Created with BioRender.com.
Treatment algorithm after HMA-VEN failure. *Combining intensive chemotherapy with a targeted agent represents an area of active research, and this treatment approach is being used off-label. **More studies are needed to assess whether adding VEN to IC can improve outcomes in the setting of post-HMA-VEN failure. BSC, best supportive care; PD, progressive disease. Created with BioRender.com.
Novel therapies in development for R/R AML
Treatment options for R/R AML, particularly after the failure of HMA-VEN, are a well-recognized area of unmet need. Clinical trials using the combination of BCL2 and MCL-1 inhibitors to overcome VEN resistance based on sound preclinical data were limited by cardiotoxicities (NCT03218683, NCT03465540, and NCT03672695).26 Navitoclax, a BCL2 and BCLXL dual inhibitor, in combination with VEN and decitabine (NCT05455294), is another potential regimen that might overcome VEN resistance; however, the severe thrombocytopenia associated with BCL-xL inhibition could be limiting. Other novel agents are being explored in early-phase trials in the R/R setting, including but not limited to small-molecule targeted inhibitors and immune-based therapies (Table 1). SNDX-5613 is a highly selective inhibitor of the menin-KMT2A interaction, which plays an essential role in regulating HOXA9, a potent transcription factor that promotes leukemogenesis.27 Menin inhibitors have been shown to promote differentiation of blast cells in MLL1(KMT2A)-rearranged or NPM1-mutated AML.28 In the first-in-human phase 1 study, 68 patients with R/R acute leukemia (n = 56 AML) were enrolled, with 89% having either an NPM1 mutation or a KMT2A rearrangement.29 The overall response rate (ORR) in the efficacy cohort (n = 60) was 53%, with NPM1 at 36% (5/14) and KMT2A at 59% (27/46). CR/CRi was 30%, with 78% of these patients achieving MRD negativity. The drug was well tolerated, and a phase 2 clinical trial is ongoing (NCT04065399). Ziftomenib is another menin inhibitor recently shown to have high response rates in patients with NPM1 mutations (a CR rate of 35% and an ORR of 45% at the recommended phase 2 dose).30 HDM201 is a potent inhibitor of the MDM2-p53 interaction and represents another promising antileukemic approach.31 The upregulation of MDM2, a ligase that degrades the tumor suppressor p53, leads to a reduction of p53 activity. In cancers with wild-type or functional p53, HDM201 promotes p53 reactivation and thereby suppresses cancer formation.31 Among 28 of the 91 R/R AML patients in a phase 1 study of HDM201, 22.2% achieved CR/CRi.32 Clinical trials using HDM201 in combination with either MBG453, an anti-TIM-3, or VEN for AML/MDS are in process (NCT03940352). FLT3 inhibitors are an important class of targeted agents with proven efficacy in select subsets of AML patients.33,34 HM43239 is a novel FLT3/SYK inhibitor that has demonstrated activity in both FLT3-mutated and wild-type AML.35 Preclinical studies suggest it can overcome resistance to prior FLT3-targeted therapy.36 In the first-in-human phase 1/2 study, 28 patients with R/R AML (FLT3-positive, 10; -negative, 16; and unknown, 2) were treated with HM43239.35 The CR/CRi rate at the expansion dose was 26.3% (5/19) with FLT3-mutated patients at 37.5% (3/8) and wild type at 18% (2/11). One of the responding patients had received gilteritinib in the past.35 This trial is currently active with a phase 2 component that combines HM43239 with VEN (NCT03850574).
Emerging novel therapies in R/R AML
| Phase | Regimen | Mechanism of action | Number of patients | Median age (range) | Response | Reference |
|---|---|---|---|---|---|---|
| 1 | SNDX-5613 | Menin inhibitor | 68 (56 R/R AML) | 51 (19-79) among adults | ORR: 53% (32/60) CR/CRi: 38% (23/60) ORR in KMT2A: 59% (27/46) ORR in NPM1: 36% (5/14) | Wang et al26 |
| 1 | HDM201 | MDM2 inhibitor | 208 (91 R/R AML) | ∼70 (23-85) | CR/CRi: 13.2% (12/91) CR/CRi in 45 mg: 22.2% (6/28) | Klossowski et al28 |
| 1/2 | HM43239 | FLT3/SYK inhibitor | 28 | 60 (35-83) | CR/CRi in 80 mg: 26.3% (5/19) CR/CRi in FLT3 80 mg: 37.5% (3/8) | Konopleva et al31 |
| 1b/2 | IMGN632 + AZA + Ven | CD123 antibody-drug conjugate | 35 (29 efficacy evaluable R/R AML) | 69 (range not available) | ORR: 55% (16/29) CR/CRi: 31% (9/29) | Daver et al35 |
| 1/2 | Magrolimab + AZA + Ven | CD47 inhibitor | 74 (29 R/R, 45 newly diagnosed) | Not available | ORR in R/R Ven-naïve: 75% ORR in R/R Ven prior: 12% | Kuruvilla et al38 |
| 1b/2 | APR-246 | p53 reactivator | 55 (11 R/R oligoblastic AML) | 66 (34-85) | ORR: 64% (n = 7) CR: 36% (n = 4) Median OS 10.8 months | Daver et al39 |
| Phase | Regimen | Mechanism of action | Number of patients | Median age (range) | Response | Reference |
|---|---|---|---|---|---|---|
| 1 | SNDX-5613 | Menin inhibitor | 68 (56 R/R AML) | 51 (19-79) among adults | ORR: 53% (32/60) CR/CRi: 38% (23/60) ORR in KMT2A: 59% (27/46) ORR in NPM1: 36% (5/14) | Wang et al26 |
| 1 | HDM201 | MDM2 inhibitor | 208 (91 R/R AML) | ∼70 (23-85) | CR/CRi: 13.2% (12/91) CR/CRi in 45 mg: 22.2% (6/28) | Klossowski et al28 |
| 1/2 | HM43239 | FLT3/SYK inhibitor | 28 | 60 (35-83) | CR/CRi in 80 mg: 26.3% (5/19) CR/CRi in FLT3 80 mg: 37.5% (3/8) | Konopleva et al31 |
| 1b/2 | IMGN632 + AZA + Ven | CD123 antibody-drug conjugate | 35 (29 efficacy evaluable R/R AML) | 69 (range not available) | ORR: 55% (16/29) CR/CRi: 31% (9/29) | Daver et al35 |
| 1/2 | Magrolimab + AZA + Ven | CD47 inhibitor | 74 (29 R/R, 45 newly diagnosed) | Not available | ORR in R/R Ven-naïve: 75% ORR in R/R Ven prior: 12% | Kuruvilla et al38 |
| 1b/2 | APR-246 | p53 reactivator | 55 (11 R/R oligoblastic AML) | 66 (34-85) | ORR: 64% (n = 7) CR: 36% (n = 4) Median OS 10.8 months | Daver et al39 |
Aside from targeted agents, immunotherapies that are antibody based are actively being explored. IMGN632 is a CD123-directed antibody-drug conjugate with the payload indolinobenzodiazepine dimer, which causes DNA alkylation.37 Synergistic effects were observed when used in combination with azacitidine and/or VEN in preclinical models.38 A phase 1b/2 study of IMGN632-AZA-VEN in R/R AML patients (n = 35) has been reported.39 Notably, over 50% had received prior VEN, and efficacy was seen across all doses and schedules. Among those evaluable for efficacy (n = 29), the ORR and CR/CRi were 55% and 31%, respectively. The CR/CRi rate was over 70% in VEN- naive, higher-intensity cohorts.39
TP53-mutated AML is a distinct disease entity with poor outcomes regardless of treatment. Compared to its wild-type counterpart, response rates are lower to any of the approved agents, and median OS is estimated to be 5 to 10 months.40 Magrolimab, a novel antibody that inhibits CD47, thereby blocking the “do not eat me” signal expressed on leukemic cells, has shown promising results even in the TP53-mutated subset.41 A total of 74 AML patients (45 newly diagnosed and 29 R/R) received magrolimab-AZA-VEN.42 Among the newly diagnosed (ORR, 80%), TP53-mutated AML patients (n = 27) had an ORR of 74%; CR/CRi, 63%; and CR, 41%. For R/R patients the ORR was 75% and 12% for VEN naive and VEN exposed, respectively. Another agent with preferential activity in TP53-mutated disease is APR-246, which works by restoring mutant p53 back to its functional conformation.41 In patients with AML (n = 11), the ORR was 64% and CR was 36%.
Other novel agents and rational drug combination studies are in the pipeline. However, it is important to note that the data for these trials, including those discussed thus far, are based upon preliminary results and small sample sizes. Larger cohorts across multiple centers in later-phase trials will help clarify and confirm the effectiveness of these regimens.
CLINICAL CASE 2 (continued)
There is no standard of care for this patient's R/R TP53- mutated AML. The preference would be enrollment in a clinical trial that utilizes a novel agent or a targeted approach. Otherwise, IC remains an option for this fit patient.
Conclusion
While the advent of HMA-VEN has transformed the treatment of patients with newly diagnosed AML, primary and acquired resistance prevent the achievement of long-term disease-free and overall survival in most patients. Signaling pathway and tumor suppressor mutations represent a major source of VEN resistance, leading to HMA-VEN treatment failure and relapse. While a subset of these patients may benefit from IC or even rechallenge with HMA-VEN, the overall prognosis is poor and options are limited. Enrollment in clinical trials with novel agents and rational combinations is needed to improve outcomes for this group of patients.
Conflict-of-interest disclosure
Onyee Chan: no competing financial interests to declare.
Alison R. Walker: no competing financial interests to declare.
Off-label drug use
Onyee Chan: Figure 2 mentions label use of intensive chemotherapy + targeted agent but doesn’t specify which agents.
Alison R. Walker: Figure 2 mentions label use of intensive chemotherapy + targeted agent but doesn’t specify which agents.
