Abstract
Immune and nonimmune microenvironmental factors play a critical role in the progression, transformation, and resistance to therapy in follicular lymphoma (FL). A recent increase in our understanding of the role of microenvironment in FL biology has led to the development of novel therapeutic strategies targeting the nonimmune and immune microenvironment. These include immunomodulatory drugs, immune checkpoint inhibitors, immnunoconjugates, and small-molecule inhibitors with an impact on the microenvironment in addition to direct antitumor activity. These agents are now at different stages of clinical development, ranging from early clinical trials in relapsed disease to phase 3 studies in the upfront setting, including combinations with other agents such as monoclonal antibodies and chemotherapy. It is important to recognize that, although the current upfront therapy of FL is associated with favorable outcomes in the majority of patients, a significant proportion experience early disease progression and develop treatment resistance and transformation to aggressive lymphoma. Although the development of “chemo-free” combinations using drugs targeting the microenvironment offers a promising approach to minimize toxicity, the identification of patients at risk of relapse and the use of biomarkers allowing the personalization of therapy will likely play a major role in the development of maintenance strategies. Against this landscape of currently available therapy options, this chapter discusses the clinical status of therapies targeting the microenvironment in FL.
Learning Objectives
To recognize the current therapy options of FL and expected outcomes
To identify the therapeutic importance of targeting the FL microenvironment
To recognize the mechanism of action and clinical activity of checkpoint inhibitors, immunomodulatory drugs, and novel immunoconjugates in FL
To recognize the impact of small-molecule inhibitors on the microenvironment and clinical activity of these agents in FL
Current therapies and prognosis of follicular lymphoma
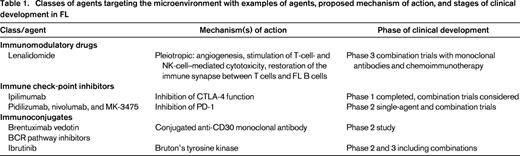
Follicular lymphoma (FL) is a low-grade lymphoma characterized by an indolent clinical course (the discussion in this chapter will be focused on FL grades 1, 2, and 3A). Despite advances in the treatment of FL, the disease remains largely incurable. Although many asymptomatic patients with low-volume disease may not require early therapy and can be observed, the majority of patients will ultimately experience disease progression and will require therapy in the course of their disease. There is no standard approach to the treatment of FL in an upfront or relapsed setting. In bulky or symptomatic disease, chemoimmunotherapy, often followed by rituximab maintenance, is frequently used, whereas patients with nonbulky or asymptomatic disease may be treated with rituximab monotherapy or simply placed on observation.1 There is a striking heterogeneity in the tempo of the disease, both in patients who are untreated and in those after treatment. Although some patients have long-term remissions lasting years if not decades, others have a rapidly progressive disease and develop treatment resistance and/or transformation to aggressive lymphoma.2,3 There is abundant evidence that the microenvironment plays a critical role in FL progression and that the assessment of the microenvironmental function and elements, including those in peripheral blood, may provide useful prognostic information.4-6 More importantly, we have recently witnessed the development of several therapies targeting the microenvironment with activity in relapsed disease. These approaches now allow for building of “chemo-free” regimens and are increasingly being evaluated in the upfront management of FL (Table 1).
Immunomodulatory agents
Lenalidomide
Lenalidomide is an oral immunomodulator with effects on immune and nonimmune microenvironments, including angiogenesis and direct antitumor activity with inhibition tumor cell proliferation. Lenalidomide has been shown to stimulate T-cell- and natural killer (NK)-cell–mediated cytotoxicity in B-cell lymphomas including FL.7 Lenalidomide was also shown to restore the immune synapse between T cells and FL B cells.8
As a single agent, lenalidomide has shown significant activity in indolent lymphoma in a single-arm, multicenter phase 2 study.9 Lenalidomide was administered at a standard dose of 25 mg on days 1-21 of 28-day cycles and continued for maximum of 52 weeks. Forty-three patients with low-grade non-Hodgkin's lymphoma (NHL) were enrolled, of whom 22 had FL. Of all of the patients, 67% were refractory to rituximab and 50% refractory to their last treatment. The overall response rate (ORR) was 27% in FL patients with a median duration of response for all of >16.5 months at data cutoff.
Lenalidomide plus rituximab (R2)
The single-agent activity of lenalidomide elicited interest in exploring lenalidomide combinations, particularly with monoclonal antibodies. In preclinical studies, lenalidomide was shown to prolong survival when combined with rituximab in a disseminated lymphoma-bearing SCID mouse xenograft model,10,11 which was also associated with an expansion of circulating NK cells and increased recruitment of NK cells to the tumor.10-12 Lenalidomide stimulated dendritic cells and altered the cytokine microenvironment, contributing to NK-cell expansion and to the augmentation of rituximab-associated antibody-dependent cellular cytotoxicity.12,13
In a pilot, single-center study of R2 [lenalidomide (Revlimid) 20 mg/d on days 1-21 of a 28-day cycle plus rituximab 375 mg/m2 on day 15 in cycle 1 and weekly for 4-8 doses] in relapsed/refractory indolent lymphoma, 8 of 9 patients with FL responded, with 5 complete responses (CRs).14 Median progression-free survival (PFS) was not reached at a median follow-up of 1 year. The Cancer and Leukemia Group B (CALGB) then conducted a phase 2 study in patients with recurrent FL and randomized them to receive lenalidomide (15 mg in cycle 1 and 20 mg in cycles 2-12 on days1-21 of 28-day cycle) alone or lenalidomide plus rituximab (375 mg/m2 weekly × 4 in cycle 1).15 All 89 evaluable patients had received rituximab-based treatment ≥6 months before the initiation of therapy. The R2 regimen demonstrated a higher response rate than single-agent lenalidomide (ORR 75% vs 49%; CR 32% vs 13%, respectively) and demonstrated significantly longer event-free survival (2.0 vs 1.2 years, respectively; P = .006).
Encouraging results in the relapsed setting led to clinical trials in an upfront setting. In a phase 2 study of previously untreated, advanced-stage indolent NHL, including FL, mantle zone lymphoma, and small lymphocytic lymphoma, patients received lenalidomide 20 mg/d on days 1-21 of a 28-day cycle (10 mg for small lymphocytic lymphoma patients) with rituximab 375 mg/m2 on day 1 of each cycle for 6 cycles. Patients with a response had an option of continuing treatment for up to 12 cycles.16 The ORR was 98% in FL with CR/unconfirmed CR (Cru) rates of 87%. Responses to R2 were independent of the Follicular Lymphoma International Prognostic Index (FLIPI) score, tumor bulk, or GELF (Groupe D'Etude des Lymphomes Folliculaires) criteria.17 The majority of patients demonstrated molecular response after completion of 3 cycles and 6 cycles of therapy with undetectable major and minor breakpoint of BCL-2 by PCR in blood and the BM. The estimated 2-year PFS was 89%. Similar results were seen in the multicenter phase 2 study of R2 in patients with previously untreated grade 1-3A FL conducted by CALGB.18 In this study of 57 evaluable patients, the ORR was 93% and the CR rate was 72%. The CR rates were again independent of FLIPI risk, histologic grade, or bulky disease. The long-term results of this trial are being evaluated.
Collectively, these studies show that R2 provides high CR rates and durable remissions in previously untreated patients with indolent NHL. Further studies evaluating the role of R2 as upfront therapy, in relapsed disease, or as maintenance therapy in FL are ongoing.
R2 combined with chemotherapy
The pleiotropic effects of lenalidomide on the lymphoma microenvironment provided a rationale for combinations of lenalidomide with chemoimmunotherapy to exploit the potential synergy of lenalidomide with cytotoxic agents. A phase 1b dose-escalation study examined first-line lenalidomide (5, 10, 15, 20, or 25 mg) given on days 1-14 in combination with standard R-CHOP21 (rituximab, cyclophosphamide, hydroxydaunorubicin, vincristine, prednisone/prednisolone for 21 days) in 27 previously untreated patients with mostly indolent NHL (18 of 27 patients with FL).19 Lenalidomide given at 25 mg daily on days 1-14 of the RCHOP21 cycle (R2-CHOP) was found to be safe and effective, with an ORR of 96% and 74% of patients having a CR/CRu. This schedule of R2-CHOP (with lenalidomide at 25 mg/d on days 1-14) was evaluated in a multicenter phase 2 study involving 80 previously untreated patients with FL grade 1-3A with high tumor burden per GELF criteria.20 R2-CHOP produced an ORR of 94% and a CR/CRu rate of 74%. During the median follow-up of 13 months, 11% of patients experienced disease progression or relapse.
An alternative attractive chemotherapy backbone for use in combination with lenalidomide in FL is BR (bendamustine and rituximab) due to its substantial activity and superior toxicity profile. The studies combining BR with lenalidomide were performed mainly in aggressive and mantle cell lymphoma, demonstrating feasibility and promising activity of this combination.21,22 There are no clinical data on the lenalidomide and BR combination in FL, and a phase 1 study evaluating this strategy in patients with relapsed low-grade lymphomas including FL is ongoing in Alliance for Clinical Trials in Oncology.
Immune checkpoint inhibition in NHL
An effective immune response is critical in the control of cancer, and immunotherapeutic approaches that promote an effective immune response have the potential to eliminate malignant cells when used as treatment. The development of protective antitumor immunity, however, is compromised by inherent immunosuppressive mechanisms and the presence of regulatory cells that often dominate the tumor microenvironment. Recent studies have shown that blocking immune checkpoints, and thereby inhibiting suppressive cells, may allow for the development of more effective antitumor immunity. This may result in effective treatment for cancer, and FL in particular. Therapeutic strategies that stimulate the immune response while simultaneously inhibiting immune suppression are a promising approach to potentially improving patient outcomes in FL.
Ipilimumab
The growth of FL cells is regulated by interactions between the malignant cell and the immune system. Cytotoxic T-lymphocyte antigen 4 (CTLA-4) is a negative regulator of T-cell function that dampens antitumor immune responses. Blocking CTLA-4 function using a monoclonal antibody directed against CTLA-4 improves immune function in a variety of different malignancies. This agent is now approved for solid tumors, including malignant melanoma, and a clinical trial in patients with relapsed and refractory B-cell NHL, including FL, showed that patients with lymphoma also respond to ipilimumab therapy. In this phase 1 trial of ipilimumab given as a single agent, 18 patients were treated and the drug was relatively well tolerated. Immune responses were seen in that T-cell proliferation to recall antigens was significantly increased in 1/3 of patients after ipilimumab treatment.23 Clinical responses were also seen in 2 patients, 1 with diffuse large B-cell lymphoma and 1 with FL. These findings confirmed that modulation of immune checkpoints may be an effective strategy in B-cell malignancies.
Anti-PD1 antibodies
The programmed cell death protein 1 (PD1) immune checkpoint pathway is used by B-cell malignancies to evade immune surveillance. PD-1 has 2 ligands, programmed cell death 1 and 2 (PD-L1 and PD-L2) belonging to B7 family of proteins. Malignant FL B cells express PD-L1, and interactions with PD1 expressed on intratumoral immune cells results in immune suppression.24 Therefore, blocking ligand activation of PD1 signaling may be a mechanism for breaking immune tolerance in FL. Clinical trials using the anti-PD1 antibody pidilizumab have shown promise in patients with diffuse large B-cell lymphoma after autologous stem cell transplantation or in combination with rituximab for relapsed and refractory patients with FL. In an international phase 2 study of pidilizumab in patients undergoing autologous stem cell transplantation, 66 patients were treated with 3 doses of pidilizumab beginning 1-3 months after transplantation.25 Treatment with pidilizumab improved the PFS, thereby meeting the primary end point of the study. At 16 months after the first treatment, the PFS was 72%. In 35 patients with measurable disease after autologous transplantation, the ORR to pidilizumab treatment was 51%.
In a second phase 2 trial using pidilizumab in combination with rituximab in relapsed FL, 32 patients received the combination. Of the 29 patients evaluable for response, 19 (66%) achieved an objective response and 52% (15 patients) had a CR to therapy.26 Additional clinical studies of other antibodies that target this pathway, including the anti-PD1 antibodies nivolumab and MK-3475, are in progress in FL patients. The alterative strategy to anti-PD1 antibodies is the development of anti-PD-L1 antibodies, currently in also in clinical studies. Treatment with immune checkpoint inhibitors appears to be a promising approach to modulating immune function in patients with FL.
Antibody drug conjugates
Antibody drug conjugates (ADCs) are an effective therapeutic option for lymphomas, and clinical activity has been seen even in lymphomas that express low levels of the antibody target. This might suggest that the drug conjugated to the antibody may have an effect on the tumor microenvironment. There may be a bystander effect targeting immune regulatory cells in addition to the direct effect of the ADC targeting the malignant cell. An anti-CD30 ADC, brentuximab vedotin, is currently being studied in patients with relapsed CD30+ B-cell NHL, including FL, with promising early results.27 Additional work needs to be done in this arena, but an effect on regulatory T cells and suppressive monocytes by ADC molecules may well contribute to the efficacy of these agents and be an additional mechanism of action.
Cell signaling inhibitors
Several small molecules inhibiting cell signaling within malignant B cells have also had a significant impact on the lymphoma microenvironment. It has been recognized that the inhibitors of the BCR pathway have an impact on both the immune and the nonimmune microenvironment.28 Although the contribution of microenvironmental effects to overall antitumor activity of these agents is difficult to assess, understanding their impact on microenvironment function is critical to the rational development of therapies combining these agents with other agents targeting the microenvironment.
BCR pathway inhibitors
Bruton's tyrosine kinase is an important component of the BCR signaling pathway. Ibrutinib is an irreversible inhibitor of Bruton's tyrosine kinase29 and has shown significant direct antitumor activity in B-cell malignances, particularly those with tonic BCR signaling (including FL).30 Ibrutinib may also have effects on the microenvironment because it has been shown to inhibit multiple cytokines and chemokines and to decrease cell migration. Ibrutinib also inhibits IL-2-inducible kinase (ITK) and thereby modulates T-cell signaling and function by preventing differentiation and activation of T helper 2 (Th2) T cells in favor of Th1 responses. The shift toward Th1 cells results a more effective antitumor immune response.31
A phase 1 study of ibrutinib in patients with relapsed and refractory NHL included 16 patients with FL with a median age of 60 years and median number of 3 prior therapies. Of these, 11 patients were treated at full dose. The ORR in these 11 patients was 55%, with 3 CRs and 3 partial responses. The median duration of response was 12.3 months and the median PFS 13.4 was months. The phase 2 study of ibrutinib in relapsed/refractory follicular is ongoing.
End points in clinical trials of agents targeting the FL microenvironment
The diverse mechanism of action of agents modulating the microenvironment requires a careful assessment of the end points in clinical studies of FL. The role of functional imaging with 18F-fluorodeoxyglucose PET in demonstrating early and late changes in the microenvironment remains to be established. Because the tumor microenvironment is responsible for a significant amount of 18F-fluorodeoxyglucose uptake, agents that cause immune activation may also cause an initial increase in PET activity (flare), similarly to effects observed in solid tumors.32 The role of minimal residual disease assessment is likely to increase, considering the effectiveness of novel therapies in inducing a molecular response.16 Finally, because the tumor response may be delayed, the identification of biomarkers of changes in the immune and nonimmune microenvironment will be critical for the successful development of clinical trials.
Future directions
This chapter focuses on therapies directly or indirectly affecting the FL microenvironment. However, many more strategies of FL therapy are in development, including novel monoclonal antibodies, bispecific antibodies, ADCs, novel small-pathway inhibitors, and innovative cell therapy approaches, including T cells with chimeric antigen receptors against malignant B-cell targets. The introduction of these new agents has dramatically expanded treatment options and will likely reduce toxicity. However, the rational incorporation of novel agents into the clinical practice of FL treatment will be a significant challenge. The majority of patients with FL will have an indolent course and studies, particularly in an upfront setting, take many years to mature. The identification of patients at risk of relapse or transformation, the development of biomarkers allowing the personalization of therapy, and the development of novel study end points will be key factors in accelerating clinical research in FL. This progress in clinical research cannot be made without patients' participation in clinical trials and the coordinated efforts of large treatment networks such as cancer cooperative treatment groups. This is a dynamic period in the treatment of FL and other lymphoid malignancies and we bear the responsibility to our patients and their families to take advantage of this progress to improve outcomes and limit toxicity.
Disclosures
Conflict-of-interest disclosures: G.S.N. has consulted for Celgene. S.M.A. declares no competing financial interests. Off-label drug use: Lenalidomide, ibrutinib.
Correspondence
Grzegorz S. Nowakowski, Mayo Clinic, 200 First St. SW, Rochester, MN 55905; Phone: (507)284-2511; Fax: (507)266-4972; e-mail: nowakowski.grzegorz@mayo.edu.