
Abstract
Case: A 65-year-old male who was previously in good health presented to his primary care physician with increasing fatigue over several months. He was found to be anemic (hemoglobin 7.5 mg/dL) and neutropenic (absolute neutrophil count 1000/μL). Further laboratory investigation showed an elevated erythropoietin level and normal iron stores. Bone marrow biopsy revealed dysplasia in two lineages and 8% blasts. Cytogenetic studies showed a clone with loss of 7q. He required red blood cell transfusions approximately every 2 weeks. He was started on hypomethylating agent treatment and referred for consultation regarding the role of hematopoietic stem cell transplantation. HLA typing results demonstrated that he had an HLA-identical sibling.
The patient in this case presented with de novo myelodysplastic syndrome (MDS), an International Prognostic Scoring System score1 of 2 (Int-2), and a WPSS (World Health Organization-adapted Prognostic Scoring System) score2 of 5 (“very high” risk category). Given his “very high” risk score by WPSS criteria, median overall survival (OS) would be expected to be 9–12 months, with a high rate of acute myelogenous leukemia (AML) transformation in 1–2 years. Although survival results may be improved by active treatment,3 there is little hope for long-term disease free survival (DFS). Hematopoietic cell transplantation (HCT) remains the only known curative treatment for MDS; however, many HCT clinical trials have been designed to exclude patients over the age of 60. In this elderly patient with preserved organ function and good performance status, is there evidence to support HCT?
To evaluate the role of HCT in patients over the age of 60 with MDS, a PubMed search was performed. The following search criteria were used: “Myelodysplastic Syndromes” [MeSH] OR “MDS” AND “Hematopoietic Stem Cell Transplantation” [MeSH] AND “Aged” [MeSH]. This initially returned 154 hits—27 reviews and 40 clinical trials. Limits were then set to Humans, Clinical Trial, Meta-Analysis, Randomized Controlled Trial, and English. Phase I trials, pharmacokinetic studies, case series, non-MDS investigations, and graft-versus-host disease (GVHD) prophylactic studies were excluded. There are no randomized controlled clinical trials evaluating the role of allogeneic HCT for the treatment of elderly (>60 years old) patients with intermediate- to high-risk MDS. The highest level of evidence is prospective cohort studies. Large retrospective reviews are the predominate form of evidence. Table 1 lists the studies included in this review and their characteristics.
Evidence-based mini-review
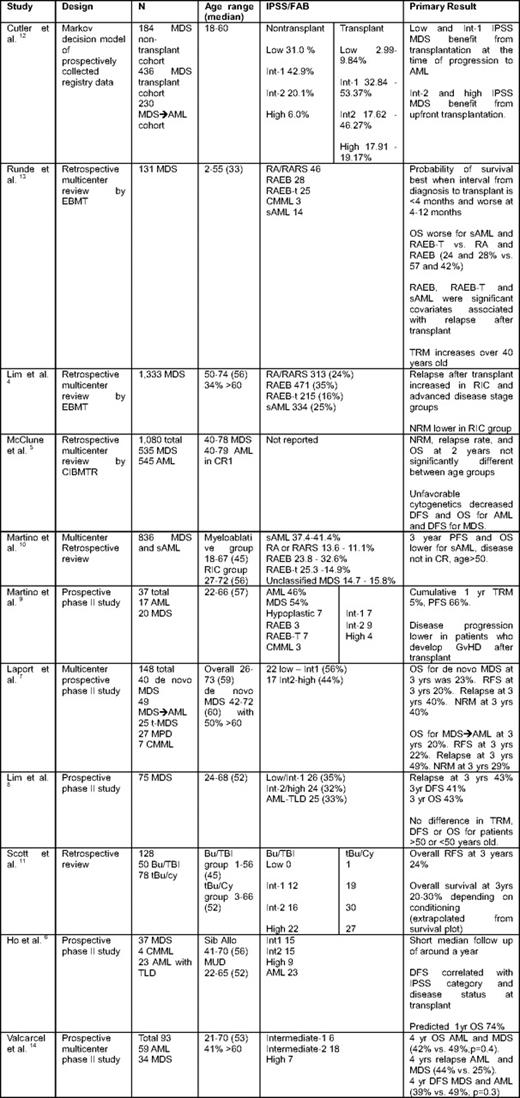
IPSS indicates International Prostate Scoring System; CIBMTR, Center for International Blood and Marrow Transplant Research; t-MDS, therapy-related MDS; CMML, chronic myelomonocytic leukemia; Bu, busulfan; TBI, total body irradiation; tBu, targeted busulfan; Cy, cytoxan; TLD, trilineage dysplasia; Sib allo, sibling allogeneic transplantation; MUD, matched unrelated donor transplantation; TRM, ??; NRM, nonrelapse mortality; CR, complete remission; GVHD, graft-versus-host disease; RFS, relapse-free survival.
Two studies address the question of age and outcomes after transplantation.4,5 Lim et al.4 retrospectively examined 1333 MDS patients over the age of 50 transplanted from 1998 to the present with either myeloablative (38%) or reduced-intensity (62%) conditioning regimens as part of the European Group for Blood and Marrow Transplantation (EBMT) registry. Thirty-four percent of patients were over the age of 60 years. In their multivariate analysis, age was not a significant factor for clinical outcomes of relapse or survival. Significant factors associated with nonrelapse mortality included type of conditioning, advanced disease at transplantation, and donor type. The 4-year OS estimate was not significantly different between those < 60 years old and those > 60 years old. However, relapse rate was increased in the > 60-year-old cohort (32% vs 41%; hazard ratio 1.32; P = .02). Finally, relapse rate and survival were significantly affected by poor-risk cytogenetics. This retrospective study suggested that age should not be a limiting factor in considering this patient for transplantation. Yet, for the case described here, cytogenetics and blast percentage > 5% put the patient at increased risk of relapse. The second study in this area by McClune et al5 included 535 MDS patients and 545 AML patients in CR1 (154 with prior MDS/myeloproliferative disease [MPD]) registered with the Center for International Blood and Marrow Transplant Research from 1995 to 2005. All transplants were reduced-intensity conditioning (RIC) or nonmyeloablative (NMA) conditioning, in contrast to the prior study. Thirty-four percent of MDS patients and 36% of AML patients were > 60 years old. In both the MDS and AML cohorts, age did not significantly affect nonrelapse mortality, DFS, or OS. Long-term disease control was seen in about one-third of MDS patients independent of age, supporting the curative potential of HCT for patients with MDS over the age of 60.
A number of studies identified in this search specifically addressed conditioning regimens for transplantation.6–11 A retrospective review of 836 MDS patients (39% over the age of 50) undergoing transplant by Martino et al10 showed that the 3-year progression free survival (PFS) and OS were similar between RIC and NMA conditioning (33% vs 39%; P = .9). The tradeoff appeared to be a decrease in nonrelapse mortality with RIC, but with an increased risk of relapse. Factors associated with a lower probability of PFS, as well as OS, included secondary AML (sAML), age > 50 years, and disease not in complete remission after AML-type chemotherapy. In a prospective multicenter study by Laport et al,7 148 patients with MDS and MPD or sAML received NMA allogeneic transplants. Forty-seven percent of patients were > 60 years old, with an age range of 26–73. Relapse at 3 years was higher in the sAML group, compared with de novo MDS (49% vs 40%); however, small numbers limited the ability to make statistical comparisons between groups. Taking three additional articles6,8,11 in sum the relapse rates at 3 years after transplant range from 34 to 43%, and OS was from 20% to 43%. These data support the curative potential of HCT for MDS, even in patients > 60 years old.
Valcarcel et al14 reported survival and relapse outcomes for homogeneously conditioned older (41% > 60 years old) patients who received allogeneic transplants for MDS or AML. Four-year OS was not statistically different between AML and MDS (42% vs 49%; P = .4). Likewise, 4-year DFS was not significantly different between MDS and AML (49% vs 39%; P = .3). The 4-year relapse rate was higher in AML (44% vs 25%). Although not a randomized controlled trial, this study suggested that patients who go on to develop sAML from MDS have a higher relapse rate posttransplant.
Timing of transplantation for MDS has been addressed by two studies. The first was based on mathematical modeling of registry databases.12 Data were prospectively collected on patients who received HLA-identical sibling transplants for MDS or sAML arising from MDS, as well on nontransplanted patients. Using a Markov analysis, Cutler and colleagues12 modeled three scenarios for newly diagnosed MDS: (1) transplant at diagnosis, (2) transplant at leukemic progression, and (3) transplant after diagnosis, but before leukemic progression. A major assumption was that 50% of patients that transform to AML from MDS would not undergo transplantation; however, a sensitivity analysis determined no significant difference in outcomes if the percentage undergoing transplantation was widely varied. Int-2 and high- risk MDS patients benefited from transplantation at diagnosis; the opposite was true for those with low and Int-1 disease. However, a major limitation of this study is that it excluded patients over the age of 60 and focused solely on myeloablative conditioning.
The final study designed to evaluate timing of transplant for MDS was a retrospective review by Runde et al13 One hundred thrity-one patients treated across 43 centers from 1983 to 1994 were identified in the EBMT registry. Patients in this cohort received tranplant from an HLA-identical sibling without induction therapy prior to the procedure. Patients were predominantly younger, with a median age of 33 years (range 2–55). DFS and OS data were provided in various subsets of FAB classifications of disease or sAML evolving from MDS. Cumulative OS for refractory anemia (RA), RA with ringed sideroblasts (RARS), RA with excess blasts (RAEBs), RA with excess blasts in transformation (RAEB-T), and sAML were 57%, 42%, 24%, and 28%, respectively. In a univariate analysis, survival was shorter for patients over the age of 40. In addition, the probability of survival was best when the interval from diagnosis to transplant was < 4 months and worse at 4–12 months. In a multivariate analysis, RAEB, RAEB-T, sAML, and disease duration > 3 months were predictors for shorter survival. Disease relapse at 5 years was highest in RAEB-T and sAML (52% and 50%, respectively), compared with RA/RARS and RAEB (13% and 44%, respectively). Multivariate analysis suggested that RAEB, RAEB-T, and sAML were significant covariates associated with relapse after transplant. DFS was highest in RA/RARS and RAEB groups, compared with RAEB-T and sAML (52%, 34%, 19%, and 26%, respectively). This study concluded that HCT “may cure approximately one-third of patients.” As in the prior study, patients over the age of 60 were not included and their analysis suggested that mortality is increased in patients over the age of 40 or if transplantation is delayed from time of diagnosis.
Conclusions
Optimal use and timing of transplantation for older patients with MDS remain an area of ongoing investigation. Based on the available evidence, we conclude that transplantation for MDS in patients aged 60 or older is the only available curative therapy, but its benefit in terms of OS has not been demonstrated in randomized controlled trials. The overall grade of recommendation for transplant for MDS over the age of 60 is grade 2B.
Disclosures
Conflict-of-interest disclosure: M.A.S. receives research funding from Genzyme and Celgene and is supported by the National Institutes of Health/National Heart, Lung and Blood Institute grant 5K12HL08710703. W.B. receives research funding from Celgene, Geron, and is supported by the National Institutes of Health/National Cancer Institute grants K23CA120708 and P50-CA140158.
Off-label drug use: Use of experimental agents in the treatment of relapsed myeloma.
Correspondence
Mark A. Schroeder, MD, Washington University in St. Louis, Division of Oncology, Section of BMT and Leukemia, 660 S. Euclid Ave., Campus Box 8007, St. Louis, MO 63110; Phone: (314) 747-8439; Fax: (314) 454-7551; e-mail: mschroed@dom.wustl.edu
