

Abstract
In multiple myeloma (MM), treatment selection and sequencing become increasingly complex with the increasing number of therapeutic options, including antibodies. Choice of treatment is dependent on various factors including patient- and tumor-related features. In addition, treatment-related factors, such as type and response to prior therapy, are also critical in terms of the selection of a new treatment regimen. Furthermore, approval status and reimbursement policies influence treatment choice. At the time of first relapse, patients who received a bortezomib-based regimen can switch to lenalidomide-based treatment, whereas patients who received lenalidomide until progression can switch to a proteasome inhibitor–based therapy. Alternatively, there is increasing evidence that pomalidomide-based triplets are also effective following the development of lenalidomide-refractory disease both in early and later relapse settings. Patients who become refractory to immunomodulatory drugs, proteasome inhibitors, and CD38 antibodies have a poor prognosis. These triple-class refractory patients may benefit from novel, recently approved agents such as XPO1 inhibitors or from participation in a clinical trial. Furthermore, retreatment with agents that were received in previous lines of therapy can also be considered in heavily pretreated patients, for example, in combination with classic cytotoxic drugs. Importantly, with the increasing use of CD38 antibodies in newly diagnosed and early relapsed/refractory MM, more information is needed on the potential value of retreatment with CD38 antibodies. With the introduction of new immunotherapies with novel modes of action, we also need a better understanding of sequencing of immunotherapeutic agents by taking into account the effect of prior therapy on immune function.
Learning Objectives
Understand the recent changes in the treatment landscape of newly diagnosed multiple myeloma
Understand how various patient-, disease-, and treatment-related features have an impact on treatment choice at diagnosis and subsequent treatment lines
Understand the activity and safety profile of approved relapse regimens for the treatment of multiple myeloma
Understand how a treatment regimen can have an impact on the subsequent line of therapy, both beneficial and detrimental, via affecting the frequency and function of immune cells
Clinical case
A 74-year-old patient with multiple myeloma (MM) was seen in the outpatient clinic for management of his first relapse. He was diagnosed with immunoglobulin G-κ MM in 2011 with bone disease, anemia, and hypercalcemia. Cytogenetic evaluation at diagnosis by fluorescence in situ hybridization showed hyperdiploidy, but no adverse-risk cytogenetic aberrations. He was enrolled in the EMN02 study and received induction therapy with bortezomib-cyclophosphamide-dexamethasone (very good partial response [VGPR] after 4 cycles), followed by high-dose melphalan (HDM) and autologous stem cell transplantation (auto-SCT). He achieved a complete response and continued with lenalidomide maintenance. In 2016, he developed progression during lenalidomide maintenance (10 mg) with a rapidly increasing M-protein and whole-body low-dose computed tomography scan that revealed new bone lesions. How should this patient be treated?
Introduction
The landscape of how to treat newly diagnosed (ND) MM (NDMM) is rapidly evolving with introduction of novel drugs and new therapeutic strategies. Based on patient and tumor characteristics, NDMM patients are treated with a combination of drugs that provides an optimal balance between anti-MM activity and safety, whereby the goal is to achieve a deep remission. To this end, I use the best drugs upfront because it has been clearly shown in several studies that introduction of new drugs in upfront regimens improves depth of response, including minimal residual disease (MRD) negativity, which translates into superior progression-free survival (PFS) and overall survival (OS), and, especially for transplant-eligible patients, the proportion of patients with operational cure.1,2 Moreover, a substantial fraction of patients do not receive second-line or third-line therapy because of death due to disease progression or therapy-related complications.3,4 This is more common in elderly patients, and those who have comorbidities and previously experienced adverse events.4 Furthermore, quality of life is best preserved during earlier therapy lines, whereas at later treatment lines, quality of life is reduced due to MM and therapy-related complications.4
Because first-line treatment dictates, in part, which therapy can be effectively given at the time of progression, I first briefly describe changes in first-line treatment of NDMM patients.
Changes in frontline treatment
Lenalidomide is increasingly used in patients with ND disease in both transplant-ineligible patients (lenalidomide-dexamethasone [Rd] and bortezomib-lenalidomide-dexamethasone [VRd]) and transplant-eligible patients (VRd induction and lenalidomide maintenance).5-8 Lenalidomide is frequently administered as continuous treatment until progression. This indicates that an increasing fraction of patients will have lenalidomide-refractory disease and prior bortezomib exposure at the time of first progression.
The second important development is the increased use of CD38 antibodies as part of first-line regimens (Table 1). CD38 antibodies were initially evaluated in heavily pretreated patients as single agents. Based on the high activity as monotherapy (at least partial response [PR], 30%) and favorable toxicity profile (mainly infusion reactions, mostly occurring during the first infusion),9 CD38 antibodies were also tested in combination with standard-of-care regimens in earlier lines of therapy. Based on these pivotal studies, several CD38 antibody-based combination therapies are now approved for the treatment of patients with both relapsed/refractory disease or NDMM (Figure 1).
Frontline phase 3 studies with CD38 antibody-based treatment
| MAIA | ALCYONE | CASSIOPEIA | GRIFFIN | |||||
|---|---|---|---|---|---|---|---|---|
| Regimen | Dara-Rd | Rd | Dara-VMP | VMP | Dara-VTd | VTd | Dara-VRd | VRd |
| HDM | HDM | HDM | HDM | |||||
| Dara-VTd | VTD | Dara-VRd | VRd | |||||
| R2: observation or dara maintenance (2 y) | R2: observation or dara maintenance (2 y) | Dara + len maintenance (Dara 2 y) | len maintenance | |||||
| No. of patients | 368 | 369 | 350 | 356 | 543 | 542 | 104 | 103 |
| Patient population | NDMM, ineligible for transplant | NDMM, ineligible for transplant | NDMM, eligible for transplant | NDMM, eligible for transplant | ||||
| ECOG PS 0-2 | ECOG PS 0-2 | ECOG PS 0-2 | ECOG PS 0-2 | |||||
| Creatinine clearance: ≥30 mL/min | Creatinine clearance: ≥40 mL/min | Creatinine clearance: ≥40 mL/min | Creatinine clearance: ≥30 mL/min | |||||
| Median follow-up, mo | 28 | 40.1 | 18.8 | 22.1 | ||||
| ≥PR | 92.9 | 81.3 | 90.9 | 73.9 | 92.6* | 89.9* | 99.0* | 91.8* |
| (s)CR | 47.6 | 24.9 | 46 | 25 | 39* | 26* | 51.5* | 42.3* |
| MRD negativity (10−5) | 24.2 | 7.3 | 28 | 7 | 64 | 44* | 51.0 | 20.4 |
| HR PFS (95% CI) | 0.56 (0.43-0.73) | 0.42 (0.34-0.51) | 0.47 (0.33-0.67) | Not reported | ||||
| Median PFS (months) | NR | 31.9 | 36.4 | 19.3 | NR | NR | NR | NR |
| HR OS (95% CI) | Not reported | 0.61 (0.46-0.80) | 0.43 (0.23-0.80) | Not reported | ||||
| Median OS (months) | NR | NR | NR | NR | NR | NR | NR | NR |
| Grade ≥ 3 neutropenia | 50.0 | 35.3 | 40† | 39† | 28 | 15 | 41 | 22 |
| Grade ≥ 3 infections | 32.1 | 23.3 | 22† | 15† | 22 | 20 | 23 | 22 |
| Grade ≥ 3 Pneumonia | 13.7 | 7.9 | 11† | 4.2† | Not reported | Not reported | 13‡ | 15‡ |
| Infusion-related reactions (all grade) | 40.9 | NA | 27.7 | NA | 35 | NA | 42 | NA |
| MAIA | ALCYONE | CASSIOPEIA | GRIFFIN | |||||
|---|---|---|---|---|---|---|---|---|
| Regimen | Dara-Rd | Rd | Dara-VMP | VMP | Dara-VTd | VTd | Dara-VRd | VRd |
| HDM | HDM | HDM | HDM | |||||
| Dara-VTd | VTD | Dara-VRd | VRd | |||||
| R2: observation or dara maintenance (2 y) | R2: observation or dara maintenance (2 y) | Dara + len maintenance (Dara 2 y) | len maintenance | |||||
| No. of patients | 368 | 369 | 350 | 356 | 543 | 542 | 104 | 103 |
| Patient population | NDMM, ineligible for transplant | NDMM, ineligible for transplant | NDMM, eligible for transplant | NDMM, eligible for transplant | ||||
| ECOG PS 0-2 | ECOG PS 0-2 | ECOG PS 0-2 | ECOG PS 0-2 | |||||
| Creatinine clearance: ≥30 mL/min | Creatinine clearance: ≥40 mL/min | Creatinine clearance: ≥40 mL/min | Creatinine clearance: ≥30 mL/min | |||||
| Median follow-up, mo | 28 | 40.1 | 18.8 | 22.1 | ||||
| ≥PR | 92.9 | 81.3 | 90.9 | 73.9 | 92.6* | 89.9* | 99.0* | 91.8* |
| (s)CR | 47.6 | 24.9 | 46 | 25 | 39* | 26* | 51.5* | 42.3* |
| MRD negativity (10−5) | 24.2 | 7.3 | 28 | 7 | 64 | 44* | 51.0 | 20.4 |
| HR PFS (95% CI) | 0.56 (0.43-0.73) | 0.42 (0.34-0.51) | 0.47 (0.33-0.67) | Not reported | ||||
| Median PFS (months) | NR | 31.9 | 36.4 | 19.3 | NR | NR | NR | NR |
| HR OS (95% CI) | Not reported | 0.61 (0.46-0.80) | 0.43 (0.23-0.80) | Not reported | ||||
| Median OS (months) | NR | NR | NR | NR | NR | NR | NR | NR |
| Grade ≥ 3 neutropenia | 50.0 | 35.3 | 40† | 39† | 28 | 15 | 41 | 22 |
| Grade ≥ 3 infections | 32.1 | 23.3 | 22† | 15† | 22 | 20 | 23 | 22 |
| Grade ≥ 3 Pneumonia | 13.7 | 7.9 | 11† | 4.2† | Not reported | Not reported | 13‡ | 15‡ |
| Infusion-related reactions (all grade) | 40.9 | NA | 27.7 | NA | 35 | NA | 42 | NA |
CR, complete response; dara, daratumumab; Dara-Rd, daratumumab-lenalidomide-dexamethasone; Dara-VMP, daratumumab-bortezomib-melphalan-prednisone; Dara-VRd, daratumumab-bortezomib-lenalidomide-dexamethasone; Dara-VTd, daratumumab-bortezomib-thalidomide-dexamethasone; HR, hazard ratio; len, lenalidomide; NA, not applicable; NR, not reached; PR, partial response; R2, second randomization; Rd, lenalidomide-dexamethasone; VMP, bortezomib-melphalan-prednisone; VRd, bortezomib-lenalidomide-dexamethasone; VTd, bortezomib-thalidomide-dexamethasone;
Response after consolidation.
During cycles 1-9.
Any grade pneumonia..
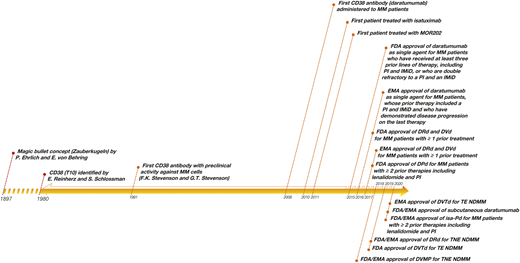
History of CD38-targeting antibodies in MM. Adapted from van de Donk et al59 with permission.
History of CD38-targeting antibodies in MM. Adapted from van de Donk et al59 with permission.
Transplant-ineligible NDMM patients can be treated with daratumumab combined with Rd or bortezomib-melphalan-prednisone (VMP) based on the results from the MAIA and ALCYONE studies, respectively. In both studies a higher frequency of deep responses, including MRD negativity, was achieved by adding daratumumab to Rd or VMP, which translated into a superior PFS.10-12 Importantly, in the ALCYONE study, there is also an OS advantage for daratumumab-VMP, compared with VMP. However, only 10% of the patients treated with VMP received a daratumumab-based regimen at the time of first relapse, which may partially explain the better survival in the daratumumab-treated group. Importantly, in both studies, patients ≥75 years of age had similar benefit from daratumumab, when compared with younger patients, which underlines the good tolerability profile of CD38 antibodies.10-12 Other studies with CD38 antibody-based regimens are under way in this patient population (eg, daratumumab or isatuximab + VRd).
Recently, the US Food and Drug Administration (FDA) and European Medicines Agency (EMA) approved the first antibody-based induction and consolidation regimen for transplant-eligible patients based on the results from the CASSIOPEIA study. This study showed that adding daratumumab to bortezomib-thalidomide-dexamethasone (D-VTd) induction before and consolidation after transplantation improves response rate and PFS.13 The GRIFFIN study showed, in a similar patient population, that daratumumab combined with VRd resulted in deeper responses, but with relatively short follow-up, not yet a PFS benefit. In Europe, the PERSEUS study is evaluating daratumumab-VRd in a larger number of transplant-eligible patients.
Second-line therapy
Although survival of MM patients has markedly improved, eventually most patients develop progressive disease. If a patient develops progression, treatment should be initiated in case of MM-related symptoms (clinical relapse) or a significant and rapid M-protein increase (eg, doubling of M-protein within 2 months; biochemical relapse).
Treatment selection and sequencing become increasingly complex with the increasing number of therapeutic options. The optimal sequence and choice of drugs is not established, and selection of treatment is dependent on patient- and tumor-related factors. Furthermore, treatment-related factors, such as type and response to prior therapy, are critical in terms of the selection of a new treatment regimen. Also, the availability of drugs, which varies considerably between countries, is an important determinant of treatment choice (Figure 2).
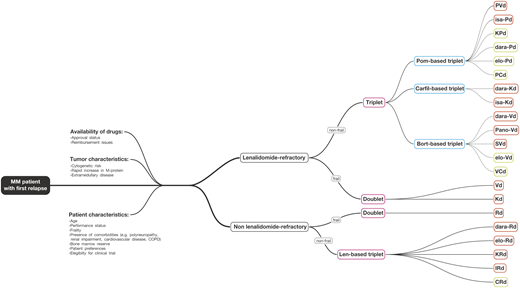
Treatment of MM patients with first relapse. Choice of treatment of patients with first relapse is dependent on patient-, tumor-, and treatment-related features. Patients, who progress on lenalidomide, can be treated with proteasome inhibitor–based therapy or a pomalidomide-based regimen. Patients who are not lenalidomide-refractory can be treated with a lenalidomide-based regimen. Alternatively, these patients may also receive retreatment with proteasome inhibitors if there is a treatment-free interval of >6 months. Regimens with red contour were evaluated in phase 3 trials; regimens with green contour were evaluated in phase 1 or 2 trials. Bort, bortezomib; Carfil, carfilzomib; CRd, cyclophosphamide-lenalidomide-dexamethasone; dara-Kd, daratumumab-carfilzomib-dexamethasone; dara-Pd, daratumumab-pomalidomide-dexamethasone; dara-Rd, daratumumab-lenalidomide-dexamethasone; dara-Vd, daratumumab-bortezomib-dexamethasone; elo-Pd, elotuzumab-pomalidomide-dexamethasone; elo-Rd, elotuzumab-lenalidomide-dexamethasone; elo-Vd, elotuzumab-bortezomib-dexamethasone; IRd, ixazomib-lenalidomide-dexamethasone; isa-Kd, isatuximab-carfilzomib-dexamethasone; Isa-Pd, isatuximab-pomalidomide-dexamethasone; Kd, carfilzomib-dexamethasone; KPd, carfilzomib-pomalidomide-dexamethasone; Len, lenalidomide; Pano-Vd, panobinostat-bortezomib-dexamethasone; PCd, pomalidomide-cyclophosphamide-dexamethasone; Pom, pomalidomide; PVd, pomalidomide-bortezomib-dexamethasone; Rd, lenalidomide-dexamethasone; SVd, selinexor-bortezomib-dexamethasone; VCd, bortezomib-cyclophosphamide-dexamethasone; Vd, bortezomib-dexamethasone.
Treatment of MM patients with first relapse. Choice of treatment of patients with first relapse is dependent on patient-, tumor-, and treatment-related features. Patients, who progress on lenalidomide, can be treated with proteasome inhibitor–based therapy or a pomalidomide-based regimen. Patients who are not lenalidomide-refractory can be treated with a lenalidomide-based regimen. Alternatively, these patients may also receive retreatment with proteasome inhibitors if there is a treatment-free interval of >6 months. Regimens with red contour were evaluated in phase 3 trials; regimens with green contour were evaluated in phase 1 or 2 trials. Bort, bortezomib; Carfil, carfilzomib; CRd, cyclophosphamide-lenalidomide-dexamethasone; dara-Kd, daratumumab-carfilzomib-dexamethasone; dara-Pd, daratumumab-pomalidomide-dexamethasone; dara-Rd, daratumumab-lenalidomide-dexamethasone; dara-Vd, daratumumab-bortezomib-dexamethasone; elo-Pd, elotuzumab-pomalidomide-dexamethasone; elo-Rd, elotuzumab-lenalidomide-dexamethasone; elo-Vd, elotuzumab-bortezomib-dexamethasone; IRd, ixazomib-lenalidomide-dexamethasone; isa-Kd, isatuximab-carfilzomib-dexamethasone; Isa-Pd, isatuximab-pomalidomide-dexamethasone; Kd, carfilzomib-dexamethasone; KPd, carfilzomib-pomalidomide-dexamethasone; Len, lenalidomide; Pano-Vd, panobinostat-bortezomib-dexamethasone; PCd, pomalidomide-cyclophosphamide-dexamethasone; Pom, pomalidomide; PVd, pomalidomide-bortezomib-dexamethasone; Rd, lenalidomide-dexamethasone; SVd, selinexor-bortezomib-dexamethasone; VCd, bortezomib-cyclophosphamide-dexamethasone; Vd, bortezomib-dexamethasone.
Several randomized phase 3 studies in patients with relapsed/refractory MM have demonstrated the superiority of triplet regimens over doublet regimens in terms of response rate and PFS. An OS benefit with a triplet regimen was observed in some studies with long follow-up. There are currently 4 lenalidomide-based triplets approved by the FDA and the EMA: 2 with an antibody as partner drug (daratumumab-Rd and elotuzumab-Rd) and 2 with a proteasome inhibitor (PI) as partner drug (carfilzomib-Rd [KRd] and ixazomib-Rd) (Table 2). Moreover, there are 3 bortezomib-dexamethasone (Vd)-based triplets approved by the FDA and the EMA: Vd plus daratumumab (DVd), pomalidomide (PVd), and panobinostat (Table 3).
Phase 3 studies evaluating Rd-based triplets in early RRMM
| POLLUX62-64 | ELOQUENT-265,66 | ASPIRE67,68 | TOURMALINE-MM115 | |
|---|---|---|---|---|
| No. of patients | 569 | 646 | 792 | 722 |
| Regimen | dara-Rd vs Rd | elo-Rd vs Rd | KRd vs Rd | IRd vs Rd |
| Patient population | • At least 1 prior line of therapy; len-refractory patients were excluded• Creatinine clearance ≥30 mL/min | • 1-3 prior lines of therapy; len-refractory patients were excluded• Creatinine clearance ≥30 mL/min | • 1-3 prior lines of therapy; len-refractory and PI-refractory patients were excluded• Creatinine clearance ≥50 mL/min | • 1-3 prior lines of therapy; len-refractory and PI-refractory patients were excluded• Creatinine clearance ≥30 mL/min |
| Prior len % / len-refractory % | 17.6 / NA | 6 / NA | 19.8 / 7.2 | 12 / 0.1 |
| Prior bort % / bort-refractory % | 84.2 / 20.6 | 70 / NA | 65.8 / 14.9 | 69 / 2* |
| CD38 antibody exposed, % | 0? | 0 ? | 0? | 0? |
| Median follow-up, mo | 44.3 | 46 | For PFS: 32.3For OS: 67.1 | 14.8 |
| ≥PR, % | 92.9 vs 76.4 | 79 vs 66 | 87.1 vs 66.7 | 78.3 vs 71.5 |
| ≥CR, % | 56.6 vs 23.2 | 5 vs 9 | 31.8 vs 9.3 | 14.2 vs 6.6 |
| HR PFS (95% CI) | 0.44 (0.35-0.55); P < .0001 | 0.71 (0.59-0.86); P = .0004 | 0.69 (0.57-0.83); P = .0001 | 0.74 (0.59-0.94); P = .01 |
| HR OS (95% CI) | HR for OS not reported; 42-mo OS: 65% vs 57% | 0.78 (0.63-0.96); P = not reported | 0.79 (0.67-0.95); P = .0045 | No OS benefit shown |
| POLLUX62-64 | ELOQUENT-265,66 | ASPIRE67,68 | TOURMALINE-MM115 | |
|---|---|---|---|---|
| No. of patients | 569 | 646 | 792 | 722 |
| Regimen | dara-Rd vs Rd | elo-Rd vs Rd | KRd vs Rd | IRd vs Rd |
| Patient population | • At least 1 prior line of therapy; len-refractory patients were excluded• Creatinine clearance ≥30 mL/min | • 1-3 prior lines of therapy; len-refractory patients were excluded• Creatinine clearance ≥30 mL/min | • 1-3 prior lines of therapy; len-refractory and PI-refractory patients were excluded• Creatinine clearance ≥50 mL/min | • 1-3 prior lines of therapy; len-refractory and PI-refractory patients were excluded• Creatinine clearance ≥30 mL/min |
| Prior len % / len-refractory % | 17.6 / NA | 6 / NA | 19.8 / 7.2 | 12 / 0.1 |
| Prior bort % / bort-refractory % | 84.2 / 20.6 | 70 / NA | 65.8 / 14.9 | 69 / 2* |
| CD38 antibody exposed, % | 0? | 0 ? | 0? | 0? |
| Median follow-up, mo | 44.3 | 46 | For PFS: 32.3For OS: 67.1 | 14.8 |
| ≥PR, % | 92.9 vs 76.4 | 79 vs 66 | 87.1 vs 66.7 | 78.3 vs 71.5 |
| ≥CR, % | 56.6 vs 23.2 | 5 vs 9 | 31.8 vs 9.3 | 14.2 vs 6.6 |
| HR PFS (95% CI) | 0.44 (0.35-0.55); P < .0001 | 0.71 (0.59-0.86); P = .0004 | 0.69 (0.57-0.83); P = .0001 | 0.74 (0.59-0.94); P = .01 |
| HR OS (95% CI) | HR for OS not reported; 42-mo OS: 65% vs 57% | 0.78 (0.63-0.96); P = not reported | 0.79 (0.67-0.95); P = .0045 | No OS benefit shown |
bort, bortezomib; CI, confidence interval; CR, complete response; dara-Rd, daratumumab-lenalidomide-dexamethasone; elo-Rd, elotuzumab-lenalidomide-dexamethasone; HR, hazard ratio; IRd, ixazomib-lenalidomide-dexamethasone; KRd, carfilzomib-lenalidomide-dexamethasone; len, lenalidomide; NA, not available; PI, proteasome inhibitor; PR, partial response; Rd, lenalidomide-dexamethasone.
Refractory to any PI.
Phase 3 studies evaluating PI-based triplets in early RRMM
| CASTOR27,69 | OPTMISSM19 | PANORAMA 170,71 | CANDOR34 | IKEMA35 | BOSTON72 | |
|---|---|---|---|---|---|---|
| No. of patients | 498 | 559 | 768 | 466 | 302 | 402 |
| Regimen | dara-Vd vs Vd | PVd vs Vd | Pano-Vd vs Vd | dara-Kd vs Kd | isa-Kd vs Kd | SVd vs Vd |
| Patient population | • At least 1 prior line of therapy; bort-refractory patients were excluded• Creatinine clearance ≥20 mL/min | • 1-3 prior lines, including ≥2 cycles of lenalidomide• Patients with severe renal impairment requiring dialysis were excluded | • 1-3 prior lines of therapy; PI-refractory patients were excluded• Creatinine clearance ≥60 mL/min | • 1-3 prior lines of therapy• Creatinine clearance ≥20 mL/min | • 1-3 prior lines of therapy• No prior therapy with carfilzomib• Creatinine clearance ≥15 mL/min | • 1-3 prior lines of therapy• At least a PR to a prior PI, if received• Creatinine clearance ≥20 mL/min |
| Prior len % / len-refractory % | 42.0 / NA | 100 / 69.9 | 20.4 / NA | 42.3 / 33.0 | NA / 32.8 | 38.3 / NA |
| Prior bort % / bort-refractory % | 65.5 / NA | 72.3 / 10.0 | 43.0 / NA | 90.3 / 29.0 | 89.7 / 33.1* | 69.4 / NA |
| CD38 antibody exposed % | 0? | 0? | 0? | 0? | 0? | 4.2 |
| Median follow-up, mo | 19.4 | 15.9 | For PFS: 6.5For OS: not reported | 16.9 | 20.7 | 13.2 and 16.5 mo in SVd and Vd arms, respectively |
| ≥PR % | 83.8 vs 63.2 | 82.2 vs 50.0 | 60.7 vs 54.6 | 84.3 vs 74.7 | 86.6 vs 82.9 | 76.4 vs 62.3 |
| (s)CR % | 28.8 vs 9.8 | 15.7 vs 4.0 | 11 vs 6 | 28.5 vs 10.4 | 39.7 vs 27.6 | 16.9 vs 10.6 |
| HR PFS (95% CI) | 0.31 (0.24-0.39);P < .0001 | 0.61 (0.49-0.77);P < .0001 | 0.63 (0.52-0.76);P < .0001 | 0.63 (0.46-0.85);P = .0014 | 0.53 (0.32-0.89);P = .007 | 0.70 (0.53-0.93);P = .0075 |
| HR OS (95% CI) | OS data immature | OS data immature; 0.98 (0.73-1.32);P = .89 | 0.94 (0.78-1.14);P = .54 | 0.75 (0.49-1.13);P = .084 | OS data immature | 0.84 (0.57-1.23);P = .19 |
| CASTOR27,69 | OPTMISSM19 | PANORAMA 170,71 | CANDOR34 | IKEMA35 | BOSTON72 | |
|---|---|---|---|---|---|---|
| No. of patients | 498 | 559 | 768 | 466 | 302 | 402 |
| Regimen | dara-Vd vs Vd | PVd vs Vd | Pano-Vd vs Vd | dara-Kd vs Kd | isa-Kd vs Kd | SVd vs Vd |
| Patient population | • At least 1 prior line of therapy; bort-refractory patients were excluded• Creatinine clearance ≥20 mL/min | • 1-3 prior lines, including ≥2 cycles of lenalidomide• Patients with severe renal impairment requiring dialysis were excluded | • 1-3 prior lines of therapy; PI-refractory patients were excluded• Creatinine clearance ≥60 mL/min | • 1-3 prior lines of therapy• Creatinine clearance ≥20 mL/min | • 1-3 prior lines of therapy• No prior therapy with carfilzomib• Creatinine clearance ≥15 mL/min | • 1-3 prior lines of therapy• At least a PR to a prior PI, if received• Creatinine clearance ≥20 mL/min |
| Prior len % / len-refractory % | 42.0 / NA | 100 / 69.9 | 20.4 / NA | 42.3 / 33.0 | NA / 32.8 | 38.3 / NA |
| Prior bort % / bort-refractory % | 65.5 / NA | 72.3 / 10.0 | 43.0 / NA | 90.3 / 29.0 | 89.7 / 33.1* | 69.4 / NA |
| CD38 antibody exposed % | 0? | 0? | 0? | 0? | 0? | 4.2 |
| Median follow-up, mo | 19.4 | 15.9 | For PFS: 6.5For OS: not reported | 16.9 | 20.7 | 13.2 and 16.5 mo in SVd and Vd arms, respectively |
| ≥PR % | 83.8 vs 63.2 | 82.2 vs 50.0 | 60.7 vs 54.6 | 84.3 vs 74.7 | 86.6 vs 82.9 | 76.4 vs 62.3 |
| (s)CR % | 28.8 vs 9.8 | 15.7 vs 4.0 | 11 vs 6 | 28.5 vs 10.4 | 39.7 vs 27.6 | 16.9 vs 10.6 |
| HR PFS (95% CI) | 0.31 (0.24-0.39);P < .0001 | 0.61 (0.49-0.77);P < .0001 | 0.63 (0.52-0.76);P < .0001 | 0.63 (0.46-0.85);P = .0014 | 0.53 (0.32-0.89);P = .007 | 0.70 (0.53-0.93);P = .0075 |
| HR OS (95% CI) | OS data immature | OS data immature; 0.98 (0.73-1.32);P = .89 | 0.94 (0.78-1.14);P = .54 | 0.75 (0.49-1.13);P = .084 | OS data immature | 0.84 (0.57-1.23);P = .19 |
bort, bortezomib; CI, confidence interval; CR, complete response; dara-Kd, daratumumab-carfilzomib-dexamethasone; dara-Vd, daratumumab-bortezomib-dexamethasone; HR, hazard ratio; isa-Kd, isatuximab-carfilzomib-dexamethasone; Kd, carfilzomib-dexamethasone; NA, not available; Pano-Vd, panobinostat-bortezomib-dexamethasone; PI, proteasome inhibitor; PR, partial response; PVd, pomalidomide-bortezomib-dexamethasone; SVd, selinexor-bortezomib-dexamethasone; Vd, bortezomib-dexamethasone.
Prior PIs/PI-refractory.
These phase 3 studies have led to the increased application of 3-drug regimens in patients with relapsed/refractory (RR) MM. However, a (dose-adjusted) doublet regimen with reduced toxicity can be the best option in frail patients. Assessment of comorbidity is also critical in selecting the best personalized treatment option for the patient. Carfilzomib is the preferred PI in patients with peripheral neuropathy, whereas this drug should be used with caution in patients with a history of cardiovascular disease.14 Dose adjustment is needed for certain drugs (eg, lenalidomide) in patients with reduced renal function to avoid toxicity. In addition, route and frequency of administration may affect quality of life and should also be considered in treatment selection. Ixazomib-Rd is an active and well-tolerated fully oral triplet combination, which may be the preferred option for elderly patients with restricted mobility or those who are working.15 Novel administration strategies may also improve convenience for patients and reduce health care burden. For example, subcutaneous daratumumab, which is recently approved, has a markedly reduced administration time (5 minutes) and results in a significant reduction in infusion-related reactions, compared with IV administration.16 Furthermore, once-weekly carfilzomib provides a more convenient dosing regimen, when compared with twice-weekly administration.17 Potent triplet regimens (eg, KRd and CD38-based regimens) are recommended in case of aggressive relapse with rapidly developing clinical symptoms. Importantly, triplet regimens also improve the outcome of patients with high-risk cytogenetic abnormalities, but poor risk is not fully abrogated.
Current treatment pathways often sequence drugs with different modes of action, but reusing a drug can also be considered based on prior response and treatment-free interval. Patients who received frontline bortezomib-based therapy can be effectively treated at the time of relapse with a lenalidomide-containing regimen, whereas patients who develop disease progression during lenalidomide treatment can receive a PI-based therapy. Furthermore, there is increasing evidence that despite acquired resistance to lenalidomide, a pomalidomide-containing regimen directly after lenalidomide can also be effective.18,19 Although cross-trial comparisons have limitations due to differences in trial design, inclusion criteria, and prior lines of therapy, a recent network meta-analysis indicates that CD38 antibody-based triplets rank among the most effective treatment options.20 The overall safety profile of CD38 antibody-based triplets is favorable, even in elderly patients.21 However, addition of a CD38 antibody to standard of care is associated with a modest increase in neutropenia and (respiratory) infections. Altogether, I favor a CD38 antibody-based regimen in patients who did not receive a CD38 antibody in prior lines of therapy, whereby the partner drugs are dependent on prior therapy: Vd (or carfilzomib-dexamethasone [Kd]/pomalidomide-dexamethasone [Pd] if available) in patients who developed lenalidomide-refractory disease and Rd in patients without lenalidomide-refractory MM.
After reinduction therapy, consolidation with high-dose therapy plus auto-SCT should be considered in patients who did not receive upfront auto-SCT, or after a previous auto-SCT with response of at least 24 months (36 months in patients who received maintenance therapy). The Myeloma X study showed that consolidation with HDM plus auto-SCT was superior to weekly cyclophosphamide after previous auto-SCT.22 In the German ReLApsE trial, there was a trend for improved PFS, as well as superior OS, in patients who received HDM plus salvage auto-SCT followed by lenalidomide maintenance, when compared with continuous treatment with Rd.23 However, the role of salvage auto-SCT in the era of continuous novel agent–based triplet therapies (effective alternatives for salvage auto-SCT in the current treatment landscape) remains unclear.
Early relapse following frontline therapy carries a very poor outcome regardless of cytogenetic risk, and, although outcomes have improved over time due to increased availability of novel classes of drugs, it still represents an unmet medical need.24,25 Allogeneic stem cell transplantation can be considered in these patients, preferentially in the setting of a clinical trial, but is associated with substantial morbidity and mortality due to infectious complications and graft-versus-host disease. Because of the rapid development of resistance to all available drugs, these patients may also benefit from new agents with novel modes of action such as novel T-cell–redirecting therapies such as B-cell maturation antigen (BCMA)-targeting chimeric antigen receptor (CAR) T cells or bispecific antibodies.
Refractory to lenalidomide
Because of the increased use of lenalidomide in NDMM, there is an increasing fraction of patients who present with lenalidomide-refractory disease at the time of first relapse (Figure 2). There is no clear data available about the efficacy of increasing the dose of lenalidomide or adding dexamethasone in patients with biochemical progression during lenalidomide maintenance.26 Furthermore, lenalidomide-refractory patients were excluded from the phase 3 trials evaluating a lenalidomide-based triplet in early RRMM. Therefore, lenalidomide-refractory patients are typically switched to a PI-based regimen. However, in several studies evaluating PI-based triplets the proportion of lenalidomide-refractory patients was very low, and specific data for patients progressing on frontline lenalidomide are not always available. The median PFS for lenalidomide-refractory patients, irrespective of number of prior treatment lines, was 8.6 months for Kd, 4.9 to 6.6 months for Vd, and 7.8 months for DVd.26 This is inferior to what is observed in the whole study population with a median PFS of 18.7 months for Kd,14 7.1 to 9.4 months for Vd,14,27 and 16.7 months for DVd.27
Importantly, the OPTMISMM study enrolled patients who were all previously lenalidomide exposed (69.9% were lenalidomide-refractory). There was a superior outcome with PVd compared with Vd in lenalidomide-refractory patients with 1 prior therapy (median PFS, 17.8 vs 9.5 months).19 The phase 3 ICARIA study also showed an advantage of a pomalidomide-containing triplet (isatuximab combined with Pd) over Pd alone in lenalidomide-refractory patients with ≥2 prior lines of therapy.28 In addition, several phase 2 studies (most in more advanced MM; Table 4) have shown activity of other pomalidomide-based combinations, such as Pd with cyclophosphamide,29 carfilzomib,30 ixazomib,31 daratumumab,18,32 or elotuzumab,33 in patients with lenalidomide-refractory disease. The EMN011 trial treated patients with refractory disease or first progression after inclusion in the EMN02 study (all patients received lenalidomide maintenance until progression in EMN02) with carfilzomib-pomalidomide-dexamethasone (KPd; median PFS, 18 months).30 A recent phase 2 study showed that sequencing daratumumab-pomalidomide-dexamethasone (DPd) immediately after development of lenalidomide-refractory disease in patients with 1 or 2 prior lines of therapy was effective.18 The ongoing phase 3 APOLLO study, which evaluates DPd, also enrolled lenalidomide-refractory patients with 1 prior line of therapy.
Randomized phase 2 and 3 studies evaluating pomalidomide-based triplets in patients with RRMM
| isa-Pd vs Pd28 | PCd vs Pd29 | elo-Pd vs Pd33 | |
|---|---|---|---|
| Phase | Randomized phase 3 | Randomized phase 2 | Randomized phase 2 |
| No. of patients | 307 | 70 | 117 |
| Median of prior lines | 3 | 4 | 3 |
| Len-refractory, % | 93 | 100 | 87 |
| Bort-refractory, % | 76* | 74 | 80* |
| Median follow-up, mo | 11.6 | Not reported | Minimum follow-up of 9.1 mo |
| ≥PR, % | 60 vs 35 | 65 vs 39 | 53 vs 26 |
| ≥VGPR, % | 32 vs 9 | 12 vs 14 | 20 vs 9 |
| Median PFS, mo | 11.5 vs 6.5 | 9.5 vs 4.4 | 10.3 vs 4.7 mo |
| Median OS, mo | 1-y OS: 72% vs 63% | Not reached vs 16.8 | Not reached in both arms |
| Approval | FDA/EMA | — | FDA/EMA |
| isa-Pd vs Pd28 | PCd vs Pd29 | elo-Pd vs Pd33 | |
|---|---|---|---|
| Phase | Randomized phase 3 | Randomized phase 2 | Randomized phase 2 |
| No. of patients | 307 | 70 | 117 |
| Median of prior lines | 3 | 4 | 3 |
| Len-refractory, % | 93 | 100 | 87 |
| Bort-refractory, % | 76* | 74 | 80* |
| Median follow-up, mo | 11.6 | Not reported | Minimum follow-up of 9.1 mo |
| ≥PR, % | 60 vs 35 | 65 vs 39 | 53 vs 26 |
| ≥VGPR, % | 32 vs 9 | 12 vs 14 | 20 vs 9 |
| Median PFS, mo | 11.5 vs 6.5 | 9.5 vs 4.4 | 10.3 vs 4.7 mo |
| Median OS, mo | 1-y OS: 72% vs 63% | Not reached vs 16.8 | Not reached in both arms |
| Approval | FDA/EMA | — | FDA/EMA |
—, no approval by FDA/EMA; Bort, bortezomib; elo-Pd, elotuzumab-pomalidomide-dexamethasone; isa-Pd, isatuximab-pomalidomide-dexamethasone; Len, lenalidomide; PCd, pomalidomide-cyclophosphamide-dexamethasone; Pd, pomalidomide-dexamethasone.
Refractory to at least 1 PI.
Kd is another backbone to which a third drug can be added to improve anti-MM activity. The CANDOR study enrolled a substantial fraction of lenalidomide-exposed or refractory patients (42.3% and 33.0%, respectively). Addition of daratumumab to Kd markedly improved the outcome of these patients.34 Similarly, addition of isatuximab to Kd significantly improved depth of response and PFS in the IKEMA study.35 No data are currently available in both studies for the subgroup of patients who progressed on frontline lenalidomide treatment. These regimens are not yet approved by FDA/EMA.
Refractory to CD38 antibody
Patients with first relapse and prior daratumumab exposure represent a growing population of patients. Although the majority of phase 3 trials evaluating triplet regimens in early relapsed MM did not enroll daratumumab-exposed patients (Tables 2 and 3), nondaratumumab-containing regimens, such as KRd or PVd, can be used to treat these patients because cross-resistance with such regimens and daratumumab is not expected. Choice of regimen is also dependent on whether the patient is progressing during treatment with other drugs (eg, lenalidomide), as well as on patient and tumor characteristics as discussed in the Second-line therapy section above.
However, there are still several open questions, including the impact of natural killer (NK)-cell depletion by daratumumab36 on a subsequent elotuzumab-containing regimen. The effect of NK-cell reduction may be limited because elotuzumab eliminates MM cells not only via NK cells, but also through a monocyte-mediated killing mechanism.
At this moment, there is not sufficient evidence to support retreatment with a CD38 antibody. Because daratumumab treatment results in CD38 reduction on the MM cell surface and depletion of NK cells, a treatment-free interval of 3 to 6 months may be needed to allow for recovery of CD38 and NK cells to baseline levels. An ongoing randomized phase 2 trial is evaluating the value of adding daratumumab to Kd in patients with prior daratumumab treatment with a treatment-free interval of ≥3 months. When considering retreatment, prior response, treatment-free interval, costs, and alternative treatment options should be taken into account.
There are also small case series showing that continuation of daratumumab, with either addition or switch in class of partner drug, may be beneficial.37-39 In addition, preclinical studies have increased our understanding of development of resistance to CD38 antibodies, which has led to the development of several interventions that are currently explored in clinical trials. This includes the administration of agents, such as all-trans retinoic acid and histone deacetylase inhibitors, which increase CD38 expression on the tumor cell surface.40 Also, adoptive transfer of CD38low NK cells, is explored as a novel strategy to enhance anti-MM activity of CD38-targeting antibodies. Furthermore, next-generation CD38-targeting drugs may be of value in case of resistance to daratumumab or isatuximab (eg, CD38 hexabodies or CD38-targeting bispecific/trispecific agents).41 Alternatively, CD38 antibody-refractory patients may also benefit from immunotherapies targeting other tumor antigens such as BCMA or GPRC5D.
Clinical case continued
Our patient developed symptomatic progression during lenalidomide maintenance therapy. Cytogenetic analysis showed that he had acquired del(17p). He had also suffered from a myocardial infarction 9 months ago, but was currently biking and walking every day in his city. Because of the poor risk conferred by del(17p) and patient’s good performance status, he started treatment with a PI-based triplet regimen. We chose a bortezomib-dexamethasone backbone because his cardiac history increases the risk of carfilzomib-related cardiovascular adverse events. As the third drug, we added daratumumab, based on the high activity of DVd in patients with first relapse. DVd is also beneficial in high-risk patients, but poor risk is not completely abrogated. With the recommended pre- and post-infusion medication, he experienced a mild infusion-related reaction during the first daratumumab infusion. When he developed mild peripheral neuropathy, we administered bortezomib once weekly instead of twice weekly, resulting in stabilization of the neuropathy. He achieved a VGPR, which lasted 2 years.
Double-refractory disease
Pd is approved for the treatment of patients with ≥2 prior lines of therapy, including lenalidomide and a PI. Activity of this regimen was significantly improved by adding a third drug. Three antibody-based regimens are currently approved in a similar patient population (DPd,32 isatuximab-Pd,28 and elotuzumab-Pd33 ). Alternatively, when these antibodies are not available, cyclophosphamide can be added to pomalidomide-dexamethasone (PCd; Table 4) or to pomalidomide-prednisone (PCP).29,42 These regimens represent a fully oral, relatively cheap treatment options.29,42
Triple-class refractory disease
Patients frequently experience multiple relapses with decreasing remission duration and length of the treatment-free interval with increasing lines of therapy.4 Eventually, patients develop disease refractory to immunomodulatory drugs (IMiDs), PIs, and CD38 antibodies (triple-class refractory), which carries a very poor survival of <12 months.45 The subgroup of patients refractory to lenalidomide, pomalidomide, bortezomib, carfilzomib, and a CD38 antibody (pentarefractory patients) has the worst outcome with a median OS of only 5.6 months.45 Because of the poor prognosis, these patients should be considered for participation in a clinical trial. Studies have shown promising results for iberdomide,46 CC-92480,47 and melflufen48 in triple-class refractory patients. In addition, belantamab mafodotin, an antibody-drug conjugate directed against BCMA, induces at least PR in 30% to 34% of triple-class refractory patients.49 Median PFS was 2.9 and 4.9 months in the 2.5 mg/kg and 3.4 mg/kg cohort, respectively.49 Furthermore, several studies with BCMA-specific CAR T cells demonstrate encouraging results in heavily pretreated MM patients. Ide-cel, a CAR T-cell product expressing a murine BCMA-targeting single-chain variable fragment, was evaluated in 128 triple-class exposed patients with at least complete response (CR) in 33% of patients and median PFS of 8.8 months.50 JNJ-4528 is a CAR T-cell therapy with 2 BCMA-targeting domains that confers high-avidity binding. Preliminary results from the CARTITUDE-1 study (29 patients; 86% triple-refractory) showed a 100% response rate with CR in 86%, and a 9-month PFS rate of 86%.51 Both CAR T-cell products received FDA breakthrough designation for RRMM. In contrast to CAR T cells, T-cell–redirecting bispecific antibodies and bispecific T-cell engager are directly “off the shelf” available. Several BCMA-targeting bispecific antibodies or BiTEs are currently evaluated in phase 1 studies with high response rates (at least PR, 67% to 89%) reported at the higher dose levels.52-54 However, patients considered for trial participation often do not fulfill the criteria for enrollment, due to aggressive relapse with development of thrombocytopenia and renal failure and necessity to start therapy directly. Also, patients with nonsecretory disease can frequently not participate in clinical trials due to absence of measurable disease.
Outside of clinical trials, these patients can now receive selinexor (an exportin-1 inhibitor) in combination with dexamethasone. This regimen was recently approved for the treatment of triple-class refractory patients by the FDA, based on a 26% overall response rate and median PFS of 3.7 months in this patient population.55 Treatment interruptions and dose reductions were common, as a result of nausea, anorexia, diarrhea, hyponatremia, thrombocytopenia, and fatigue. Alternatively, retreatment with agents that were received in previous lines of therapy can be considered in heavily pretreated patients, especially after a long-lasting remission and in combination with other drugs. The combination of novel agents with classic cytotoxic drugs, such as cyclophosphamide, anthracyclines, or bendamustine, can also be effective in patients with advanced MM. For example, lenalidomide combined with continuous low-dose oral cyclophosphamide and prednisone is effective and well tolerated in lenalidomide-refractory MM patients (at least PR, 67%; median PFS, 12.1 months).56
Sequencing immunotherapy
With the increasing use of immunotherapy in MM, more studies are needed to increase our understanding of the best sequence of anti-MM drugs to maximize patient benefit. PIs, alkylating drugs, and steroids reduce the number and function of T cells, and thereby these agents potentially reduce the activity of subsequent therapy with T-cell–engaging bispecific antibodies. Exposure to these drugs can also reduce the fitness of T cells in the apheresis product and thereby impair the efficacy of CAR T-cell therapy. In contrast, preclinical studies have shown that prior daratumumab treatment enhances the efficacy of BCMA-targeting T-cell engaging bispecific antibodies by virtue of its immunomodulatory effects, such as the elimination of CD38+ regulatory T cells and myeloid-derived suppressor cells.57-59 On the other hand, because activated T cells upregulate CD38, antibodies targeting CD38 may also have a negative impact on these cells. However, we have previously demonstrated that daratumumab treatment results in a rapid downregulation of CD38 on T cells, which is mediated through the trogocytic transfer of CD38/daratumumab complexes from T cells to monocytes and granulocytes.60 Despite reducing CD38 expression on T cells, daratumumab promotes T-cell expansion and increases their functional activity.58,60 Ongoing studies will demonstrate whether CD38 antibodies can be effectively combined with T-cell–redirecting therapies. The immune-stimulating effects of daratumumab, which possibly persist into the subsequent line of therapy because of its long half-life,57 may also explain the efficacy of retreatment with an IMiD following development of progression during daratumumab.61 Importantly, IMiDs can still be immune stimulating, when the tumor is resistant to the drug.56 Improved understanding of the impact of prior therapy on subsequent immunotherapy will also be relevant when T-cell–redirecting therapy will be used as part of first-line therapy (eg, to convert patients from MRD+ to MRD−). Another open question is the impact of reducing tumor burden prior to T-cell–redirecting therapy (optimizing effector-to-target ratio). More information is also needed about the best treatment strategy for patients relapsing after BCMA-targeted therapy: how effective is sequencing of agents that target BCMA vs using immunotherapies targeting other tumor antigens such as GPRC5D or SLAMF7? We also need clinical trials to evaluate novel combinations of immunotherapeutic agents. This includes studies to find the best partner drug for bispecific antibodies and to evaluate drugs that can improve the persistence of CAR T cells without increasing toxicity, such as cytokine-release syndrome. Potential candidates include T-cell stimulatory agents such as IMiDs, iberdomide, and CD38 antibodies.
Conclusions
Treatment selection and sequencing become more and more complex with the increasing number of therapeutic options that are available in MM. Also, the increased use of lenalidomide and CD38 antibodies as part of first-line regimens has major impact on treatment of first relapse. There are several important open questions, such as whether patients with prior exposure to CD38 antibodies can be retreated with or without a washout period. Furthermore, because of the introduction of new agents with a novel mechanism of action (such as T-cell–redirecting agents) we need a better understanding of how all available drugs can be sequenced in the most optimal way to maximize patient survival and minimize toxicity. Because of the introduction of new immunotherapies in MM, sequencing should, more than ever, take into account the potential harmful or beneficial impact of drugs on the immune microenvironment, and how that influences the efficacy of subsequent lines of therapy.
Correspondence
Niels W. C. J. van de Donk, Department of Hematology, Cancer Center Amsterdam, Vrije Universiteit Amsterdam, Amsterdam UMC, De Boelelaan 1117, 1081 HV, Amsterdam, The Netherlands; e-mail: n.vandedonk@amsterdamumc.nl.
