

Abstract
Immunodeficiency, whether acquired in the case of human immunodeficiency virus (HIV) infection or congenital due to inborn errors of immunity (IEIs), presents clinically with not only infection and immune dysregulation but also increased risk of malignancy. The range of malignancies seen is relatively limited and attributable to the particular cellular and molecular defects in each disease. CD4+ T-cell lymphopenia in people living with HIV infection (PLWH) and certain IEIs drive the predisposition to aggressive B-cell non-Hodgkin lymphomas, including certain rare subtypes rarely seen in immunocompetent individuals. PLWH and IEI that lead to profound T-cell lymphopenia or dysfunction also are at risk of cancers related to oncogenic viruses such as Kaposi sarcoma herpesvirus, Epstein-Barr virus, human papillomavirus (HPV), and Merkel cell polyomavirus. IEIs that affect natural killer cell development and/or function heavily predispose to HPV-associated epithelial cancers. Defects in DNA repair pathways compromise T- and B-lymphocyte development during immune receptor rearrangement in addition to affecting hematopoietic and epithelial DNA damage responses, resulting in both hematologic and nonhematologic cancers. Treatment of cancers in immunodeficient individuals should be curative in intent and pursued in close consultation with disease experts in immunology and infectious disease.
Learning Objectives
Understand the immunologic defects in PLWH infection and their relationship to the development of cancer
Recognize that IEIs affecting lymphocytes and/or DNA repair predispose to cancer
CLINICAL CASE 1, PART 1
A 28-year-old cisgender man who immigrated to the United States from Uganda 10 years ago presents to the emergency room with shortness of breath. He also reports 6 months of weight loss, fatigue, and fevers. On examination, the patient is in respiratory distress and has raised, violaceous plaques on his trunk and extremities. Chest x-ray reveals a large left-sided pleural effusion. The patient undergoes testing for human immunodeficiency virus (HIV), which is positive. His HIV viral load is 150 000 copies/mL, with a CD4+ T-cell count of 110 cells/µL. After consultation with an HIV specialist and a pharmacist, the patient is started on combination antiretroviral therapy (ART) including bictegravir, emtricitabine, and tenofovir alafenamide along with sulfamethoxazole/trimethoprim and valacyclovir for opportunistic infection prophylaxis. Biopsy specimen of one of the skin lesions is consistent with Kaposi sarcoma (KS). Preliminary results from a therapeutic and diagnostic thoracentesis indicate a B-cell lymphoma. Further pathologic workup indicates the malignant B cells are negative for CD20 and CD19 and positive for CD138, CD38, and CD45, as well as both Kaposi sarcoma herpesvirus (KSHV) and Epstein-Barr virus (EBV), indicating a diagnosis of primary effusion lymphoma (PEL).
Cancers arising in people with HIV/AIDS
Cancer and HIV/AIDS have been linked since the first cluster of cases of KS and pneumocystis pneumonia were reported in 1981. It was soon recognized that people living with HIV (PLWH) were susceptible to other cancers, particularly aggressive B-cell non-Hodgkin lymphomas (NHLs) (Table 1).1 With the discovery of KSHV (also called human herpesvirus 8) in 1994 and its subsequent finding as the causative agent of KS, it became apparent that many, but not all, HIV- associated cancers are caused by oncogenic viruses.2
Etiology and incidence of cancers among PLWH
| Etiologic virus | Cancer type | Role of immunosuppression | Other risk factors | SIR in the United States3,4 | Comment |
|---|---|---|---|---|---|
| KSHV | Kaposi sarcoma | +++ | Men who have sex with men | 498 | Very common in parts of sub-Saharan Africa |
| EBV | Non-Hodgkin lymphoma* | ++ to ++++ | HBV, HCV | 12 | |
| Hodgkin lymphoma | ++ | Male sex | 7.7 | Mixed cellularity is most common subtype | |
| HPV | Anal cancer | + | Tobacco, anal warts | 19 | Incidence increasing |
| Cervical cancer | + | Tobacco | 3.2 | Very common in resource-limited regions | |
| Oropharyngeal cancer | + | Tobacco, alcohol | 1.6-2.2† | Incidence increasing | |
| Vulvar cancer | + | Tobacco | 9.4 | ||
| Penile cancer | + | Tobacco, lack of circumcision | 5.3 | ||
| HBV, HCV | Hepatocellular cancer | + | Alcohol, cirrhosis | 3.2 | |
| MCPyV | Merkel cell carcinoma | + | Sun exposure | 2.6 | At least 15% of cases not associated with MCPyV |
| None or unknown | Lung cancer | + | Tobacco, pulmonary infections | 2 | Most common cancer-related cause of death |
| Nonmelanoma skin cancer | + | Sun exposure, family history | 2.1 | ||
| Conjunctival carcinoma | + | Sun exposure | 5.5 | Rare in the United States; occurs most often in sub-Saharan Africa; viral etiology suspected |
| Etiologic virus | Cancer type | Role of immunosuppression | Other risk factors | SIR in the United States3,4 | Comment |
|---|---|---|---|---|---|
| KSHV | Kaposi sarcoma | +++ | Men who have sex with men | 498 | Very common in parts of sub-Saharan Africa |
| EBV | Non-Hodgkin lymphoma* | ++ to ++++ | HBV, HCV | 12 | |
| Hodgkin lymphoma | ++ | Male sex | 7.7 | Mixed cellularity is most common subtype | |
| HPV | Anal cancer | + | Tobacco, anal warts | 19 | Incidence increasing |
| Cervical cancer | + | Tobacco | 3.2 | Very common in resource-limited regions | |
| Oropharyngeal cancer | + | Tobacco, alcohol | 1.6-2.2† | Incidence increasing | |
| Vulvar cancer | + | Tobacco | 9.4 | ||
| Penile cancer | + | Tobacco, lack of circumcision | 5.3 | ||
| HBV, HCV | Hepatocellular cancer | + | Alcohol, cirrhosis | 3.2 | |
| MCPyV | Merkel cell carcinoma | + | Sun exposure | 2.6 | At least 15% of cases not associated with MCPyV |
| None or unknown | Lung cancer | + | Tobacco, pulmonary infections | 2 | Most common cancer-related cause of death |
| Nonmelanoma skin cancer | + | Sun exposure, family history | 2.1 | ||
| Conjunctival carcinoma | + | Sun exposure | 5.5 | Rare in the United States; occurs most often in sub-Saharan Africa; viral etiology suspected |
See Figure 2.
SIR is 1.6 for HPV-related cancers and 2.2 for HPV-unrelated cancers.
SIR, standardized incidence ratio; +, low; ++, moderate; +++, significant; ++++, very significant role for immunosuppression in pathogenesis.
HIV infects CD4+ T cells and certain other cell types, and the primary immune defect is CD4+ T-cell lymphopenia. HIV infection also causes other disruptions of immune function, including depletion of other lymphocyte populations, defects in lymphocyte function, increased inflammatory cytokines, and chronic inflammation. These immunologic defects impair control of oncogenic viruses, such as KSHV, EBV, human papillomavirus (HPV), and Merkel cell polyomavirus (MCPyV), leading to the development of cancer (Table 1, Figure 1). KSHV is an essential cause of KS, and populations with a higher prevalence of KSHV infection experience higher rates of KS, such as men who have sex with men and those living in certain areas of sub-Saharan Africa. PLWH also have a higher exposure to high-risk types of HPV, increasing the risk for cervical and anal cancer. Increased rates of tobacco use and infection with hepatitis B virus (HBV) and hepatitis C virus (HCV) also contribute to higher cancer rates in PLWH (Table 1).
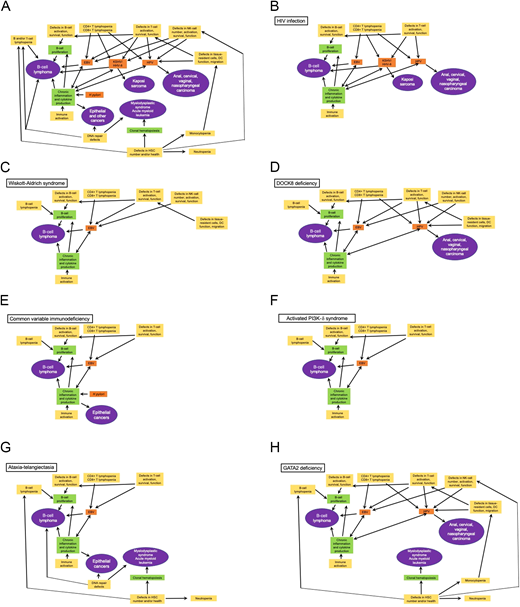
Key relationships between immune defects and oncogenesis. General relationships are shown in A, and key relationships specific to the indicated diseases are shown in B-H. Yellow boxes denote key immunologic defects observed in HIV/AIDS and/or IEI; green boxes denote secondary defects; orange boxes denote infectious agents that contribute to malignancies in immunodeficiency; purple ovals show the principal malignancies associated with the immune defects. DC, dendritic cell; HHV-8, human herpesvirus 8.
Key relationships between immune defects and oncogenesis. General relationships are shown in A, and key relationships specific to the indicated diseases are shown in B-H. Yellow boxes denote key immunologic defects observed in HIV/AIDS and/or IEI; green boxes denote secondary defects; orange boxes denote infectious agents that contribute to malignancies in immunodeficiency; purple ovals show the principal malignancies associated with the immune defects. DC, dendritic cell; HHV-8, human herpesvirus 8.
The development of an effective 3-drug ART in the mid-1990s allowed for meaningful restoration of CD4+ T-cell counts, and AIDS was converted from a death sentence to a chronic disease. ART substantially reduced the incidence of the cancers associated with profound immunodeficiency such as KS and certain B-cell lymphomas. However, as PLWH live longer, they have an increased cumulative likelihood of developing cancers associated with moderate decreases in CD4+ T-cell counts (Table 1). PLWH also remain at risk of cancers not associated with immunodeficiency. In fact, cancer is now one of the most common or the most common cause of death in PLWH in regions where ART is readily available. Interestingly, PLWH do not have an increased incidence of certain common cancers, such as breast, colon, and prostate cancer; however, they may present at more advanced stages or with more aggressive subtypes.5,6
NHL is the most common cancer among PLWH in the United States.3 NHL is associated with moderate to severe immunosuppression depending on the subtype (Figure 2). Hodgkin lymphoma is also increased but generally occurs at preserved CD4+ T-cell counts and is associated with use of ART.7 Diffuse large B-cell (DLBCL) is the most common NHL subtype in PLWH, followed by Burkitt lymphoma and rare subtypes occurring almost exclusively in PLWH, particularly PEL and plasmablastic lymphoma. The incidence of primary central nervous system lymphoma, which is associated with profound immunosuppression, drastically declined with the advent of ART and remains rare. Lymphoma often presents at advanced stages in PLWH with more rapid progression, frequent B symptoms, and frequent involvement of extranodal sites and the central nervous system than the general population.8 The depth of the CD4+ nadir, uncontrolled HIV viremia, and interruptions in ART are all associated with increased risk of NHL.9-11 A relatively large percentage of HIV-associated lymphomas is associated with EBV, including almost 100% of primary central nervous system lymphomas.12 KSHV is the causative agent of PEL, but most are also coinfected with EBV. Chronic B-cell activation in PLWH contributes to lymphomagenesis, and coinfection with HBV and/or HCV may also increase the risk of NHL through this mechanism.13

Pathologic, immune, and viral characteristics of HIV-associated NHL. ABC, activated B cell; GCB, germinal center B cell; IRF4, interferon regulatory factor 4; MUM1, multiple myeloma 1; PBL, plasmablastic lymphoma. *Indicates MYC gene rearrangements. This figure was created on biorender.com.
Pathologic, immune, and viral characteristics of HIV-associated NHL. ABC, activated B cell; GCB, germinal center B cell; IRF4, interferon regulatory factor 4; MUM1, multiple myeloma 1; PBL, plasmablastic lymphoma. *Indicates MYC gene rearrangements. This figure was created on biorender.com.
As exemplified by case 1, patients with malignancies that are more frequent in HIV/AIDS should be screened for HIV infection, especially if they are in a high-risk group. Before the development of effective ART, treatment with curative-intent chemotherapy for HIV-associated malignancies was nearly impossible given the profound immunosuppression and risk of infectious complications. With ART, it has been shown that most cancers arising in PLWH are best treated with the same regimens used to treat HIV- negative patients.14,15 The National Comprehensive Cancer Network has published practice guidelines for cancer in people with HIV, HIV-related NHL, and KS. PLWH should continue ART while undergoing cancer therapy, and oncologists should work closely with HIV specialists to ensure optimal HIV management and infection prophylaxis. Oncologists should consult with pharmacists to avoid drug-drug interactions, especially if patients are taking HIV protease inhibitors, which are metabolized by the cytochrome P450 enzymes. One of the most exciting developments in cancer therapy is the success of immune checkpoint inhibitors targeting PD-1, PD-L1, or CTLA-4. Despite initial toxicity and efficacy concerns, recent studies have shown them to be safe and effective in expected cancer types in PLWH with more than 100 CD4+ T cells/µL.16 It should be stressed that HIV infection is a chronic, manageable condition, and US Food and Drug Administration guidance endorses inclusion of PLWH with 350 or more CD4+ cells/µL for all cancer clinical trials as well as their inclusion at lower CD4+ T cell counts if patients have potentially curable malignancies or if the study agents have been shown to have activity in a given cancer.17 PLWH treated for cancer are at increased risk for secondary primary cancers, further underscoring the need for vigilance and adherence to cancer screening guidelines.18
CLINICAL CASE 1, PART 2
For the patient's PEL, an oncologist prescribes curative-intent treatment with dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin (EPOCH) in addition to continuing ART. After 6 cycles of EPOCH, the patient's lymphoma is in complete remission, his CD4+ T cell count is 90 cells/µL, and his HIV viral load is undetectable. Two months later, the patient develops increasing numbers of nodular KS lesions on his lower extremities. His oncologist prescribes liposomal doxorubicin to treat the KS while the patient's immune system reconstitutes following EPOCH. After 4 cycles, there is significant flattening and lightening of the KS lesions, and liposomal doxorubicin is discontinued. One year following EPOCH treatment, the patient's PEL is in remission, the cutaneous KS lesions are barely visible, CD4+ T-cell count is 350 cells/µL, and HIV viral load remains undetectable.
CLINICAL CASE 2
A 25-year-old man with a history of recurrent respiratory tract infections was referred to an immunologist for evaluation. He was found to have dysgammaglobulinemia, poor antigen-specific responses, hyper-IgM, and IgA deficiency, consistent with a diagnosis of common variable immunodeficiency. Suspecting an inborn error of immunity (IEI), the immunologist ordered whole-exome sequencing. While awaiting further testing, the patient presented to a local emergency room with cervical lymphadenopathy and a mediastinal mass and was treated with emergent corticosteroids. The biopsy specimen was initially read as Hodgkin lymphoma, but his immunologist questioned the diagnosis and requested EBV testing of the tumor. Rereview of pathology found that what were thought to be Reed-Sternberg cells were large atypical cells that had completely effaced the nodal architecture and were positive for EBV, CD20, PAX5, and CD30, consistent with EBV+ DLBCL lymphoma. Whole-exome sequencing showed a heterozygous E1021K variant in the PIK3CD gene. After further lymphoma treatment, he underwent successful allogeneic transplantation with a matched unrelated donor.
Cancers arising in people with IEIs
Advances in genetics have led to a veritable explosion of defined primary immunodeficiency diseases, now termed IEIs. The International Union of Immunological Societies (IUIS) currently lists more than 450 diseases, categorized broadly into 10 phenotypic groups (Table 2).19-21 The speed with which these disorders are being described is evident by the number of disorders in each biennial publication (191 in 2011, 430 in 2019) and the fact that the 2019 meeting report, published in January 2020, was sufficiently outdated that a supplement adding 26 additional monogenic gene defects was published in January 2021.
IEIs associated with malignancies
| Number | IUIS category | Examples | Associated malignancies | ||||
|---|---|---|---|---|---|---|---|
| B- or T-cell lymphomas (reference) | HPV-driven cancers | Myelodysplastic syndrome and/or myeloid leukemia | Gastric adenocarcinoma or lymphoma | Other | |||
| 1 | Immunodeficiencies affecting cellular and humoral immunity | SCID | SCID (ADA, RAG1, LIG4, DCLRE1C, coronin 1a) ZAP70 | — | — | — | OX40 deficiency (KS) CD40L (cholangio carcinoma) |
| 2 | Combined immunodeficiencies with associated or syndromic features | WAS Ataxia- telangiectasia | WAS DOCK8 deficiency CARD11 autosomal dominant loss of function Ataxia-telangiectasia Nijmegen breakage syndrome Bloom syndrome Immunodeficiency with centromeric instability and facial anomalies Schimke immuno- osseous dysplasia Cartilage hair hypoplasia DiGeorge syndrome CHARGE syndrome PNP deficiency | — | — | Ataxia-telangiectasia | Ataxia-telangiectasia (breast, thyroid, liver, brain, acute lymphoblastic leukemia) |
| 3 | Predominantly antibody deficiencies | CVID | APDS CVID Selective IgA deficiency | — | — | CVID Selective IgA deficiency | — |
| 4 | Diseases of immune dysregulation | ALPS IPEX HLH | ALPS X-linked lymphoproliferative disease type 1 XMEN ITK deficiency CD27/CD70 deficiency CTPS1 deficiency IL10R deficiency | — | — | — | — |
| 5 | Congenital defects of phagocyte number or function | Chronic granulomatous disease Severe congenital neutropenia Leukocyte adhesion deficiency | — | GATA2 deficiency | GATA2 deficiency Severe congenital neutropenia (ELANE, HAX1, other) Shwachman-Diamond syndrome X-linked neutropenia due to gain of function mutations in WAS SMARCAD2 | — | — |
| 6 | Defects in intrinsic and innate immunity | IL-12 and interferon γ pathway defects | WHIM syndrome | Epidermodysplasia verruciformis WHIM syndrome | — | — | — |
| 7 | Autoinflammatory disorders | Familial Mediterranean fever Aicardi-Goutieres syndrome | — | — | — | — | — |
| 8 | Complement deficiencies | Hereditary angioedema | — | — | — | — | — |
| 9 | Bone marrow failure | Fanconi anemia Dyskeratosis congenita | Dyskeratosis congenita | — | Fanconi anemia Dyskeratosis congenita Coats plus syndrome MIRAGE (SAMD9) Ataxia pancytopenia syndrome (SAMD9L) | — | Fanconi anemia (breast, skin, head and neck, other) |
| 10 | Phenocopies of IEI | Somatic mutations leading to ALPS RAS- associated autoimmune leukopro- liferative disease | — | — | — | — | — |
| Number | IUIS category | Examples | Associated malignancies | ||||
|---|---|---|---|---|---|---|---|
| B- or T-cell lymphomas (reference) | HPV-driven cancers | Myelodysplastic syndrome and/or myeloid leukemia | Gastric adenocarcinoma or lymphoma | Other | |||
| 1 | Immunodeficiencies affecting cellular and humoral immunity | SCID | SCID (ADA, RAG1, LIG4, DCLRE1C, coronin 1a) ZAP70 | — | — | — | OX40 deficiency (KS) CD40L (cholangio carcinoma) |
| 2 | Combined immunodeficiencies with associated or syndromic features | WAS Ataxia- telangiectasia | WAS DOCK8 deficiency CARD11 autosomal dominant loss of function Ataxia-telangiectasia Nijmegen breakage syndrome Bloom syndrome Immunodeficiency with centromeric instability and facial anomalies Schimke immuno- osseous dysplasia Cartilage hair hypoplasia DiGeorge syndrome CHARGE syndrome PNP deficiency | — | — | Ataxia-telangiectasia | Ataxia-telangiectasia (breast, thyroid, liver, brain, acute lymphoblastic leukemia) |
| 3 | Predominantly antibody deficiencies | CVID | APDS CVID Selective IgA deficiency | — | — | CVID Selective IgA deficiency | — |
| 4 | Diseases of immune dysregulation | ALPS IPEX HLH | ALPS X-linked lymphoproliferative disease type 1 XMEN ITK deficiency CD27/CD70 deficiency CTPS1 deficiency IL10R deficiency | — | — | — | — |
| 5 | Congenital defects of phagocyte number or function | Chronic granulomatous disease Severe congenital neutropenia Leukocyte adhesion deficiency | — | GATA2 deficiency | GATA2 deficiency Severe congenital neutropenia (ELANE, HAX1, other) Shwachman-Diamond syndrome X-linked neutropenia due to gain of function mutations in WAS SMARCAD2 | — | — |
| 6 | Defects in intrinsic and innate immunity | IL-12 and interferon γ pathway defects | WHIM syndrome | Epidermodysplasia verruciformis WHIM syndrome | — | — | — |
| 7 | Autoinflammatory disorders | Familial Mediterranean fever Aicardi-Goutieres syndrome | — | — | — | — | — |
| 8 | Complement deficiencies | Hereditary angioedema | — | — | — | — | — |
| 9 | Bone marrow failure | Fanconi anemia Dyskeratosis congenita | Dyskeratosis congenita | — | Fanconi anemia Dyskeratosis congenita Coats plus syndrome MIRAGE (SAMD9) Ataxia pancytopenia syndrome (SAMD9L) | — | Fanconi anemia (breast, skin, head and neck, other) |
| 10 | Phenocopies of IEI | Somatic mutations leading to ALPS RAS- associated autoimmune leukopro- liferative disease | — | — | — | — | — |
CHARGE, coloboma, heart anomaly, choanal atresia, retardation, genital and ear anomalies; HLH, hemophagocytic lymphohistiocytosis; IPEX, immune dysregulation, polyendocrinopathy, enteropathy, X-linked; MIRAGE, myelodysplasia, infection, restriction of growth, adrenal hypoplasia, genital phenotypes, and enteropathy; PNP, purine nucleoside phosphorylase; RAS, rat sarcoma; SCID, severe combined immunodeficiency; WHIM, warts, hypogammaglobulinemia, infections, and myelokathexis.
At least 10% of IEIs are stated within the IUIS reports to be associated with malignancies. The distribution of IEIs associated with malignancy is not even with respect to category; very few fall into the categories of defects in intrinsic and innate immunity, complement defects, and autoinflammatory disorders.22,23 As reviewed below, distinct and overlapping mechanisms are responsible for a predisposition to malignancy among patients with IEIs (Figure 1).
General pathogenic mechanisms
As in HIV/AIDS, T-cell lymphopenia and dysfunction generally predispose to both poor tumor surveillance and opportunistic infection with oncogenic viruses. T-cell dysfunction may lead to dysregulated proliferation of B cells, which may be further exacerbated by conditions that lead to B-cell lymphopenia or intrinsically aberrant B-cell signaling.
Natural killer (NK) cells are critical for control of certain viruses, particularly DNA viruses such as HPV and EBV. Control of viral infections in skin or tissue is often dependent on antigen presenting cells such as monocytes and dendritic cells, which must undergo activation, changes in shape, and migration through tissues to interact with T cells and traffic to secondary lymphoid organs.
Mutations in a host of genes involved in DNA repair predispose to lymphoid malignancy and epithelial malignancy, due to the general need for faithful DNA repair in all tissues. Repair of double-stranded breaks generated in the T-cell receptor and immunoglobulin loci by RAG1/RAG2 depends on the nonhomologous end-joining pathway. Thus, defects in genes such as LIG4, DCLRE1C, XLF1, and NBS1 tend to result in T- and B-cell lymphopenia and furthermore increase the chance of translocations associated with lymphoma. Outside of lymphocytes, mutations in these genes and others involved in homologous recombination and the response to DNA damage (eg, BLM, the gene mutated in Bloom syndrome) render the patients radiation sensitive. Oncogenesis is common particularly in rapidly dividing tissues, including skin, gastrointestinal tract, breast, genitourinary tract, soft tissues, and bone marrow.
Defects of hematopoietic stem cell (HSC) fitness, differentiation, and/or survival contribute to bone marrow failure, in the setting of replicative stress and clonal hematopoiesis of a limited pool of HSCs. Accumulation of additional mutations promotes the development of myelodysplasia and ultimately acute myeloid leukemia. In these disorders (eg, Shwachman-Diamond syndrome, dyskeratosis congenita, or severe congenital neutropenia), the immunodeficiency is typically related to neutropenia rather than defects of lymphocytes or adaptive immunity.
Individual disorders with more than 1 mechanism involved
Wiskott-Aldrich syndrome and dedicator of cytokinesis 8 deficiency
Wiskott-Aldrich syndrome (WAS) is an X-linked disorder caused by mutations in the WAS gene, resulting in a syndrome of microthrombocytopenia, eczema, infections, autoimmunity, and predisposition to lymphoma. WAS protein is critical for actin cytoskeletal rearrangement, which in turn is required for formation of the immune synapse in response to T, B, and NK cell-cell signaling, for regulatory T-cell function, monocyte cytokine production, and lymphocyte and dendritic cell shape and mobility.24 Progressive CD8+ T-cell lymphopenia, impaired T cell receptor signaling and activation, poor NK cell function, overactive B cell receptor signaling, and dysregulated monocyte activation all conspire to promote lymphomagenesis with and without EBV infection (Figure 1).
Dedicator of cytokinesis 8 (DOCK8) deficiency is an autosomal recessive disorder that shares features with WAS, including eczema, infections, and autoimmunity, but also is characterized by herpetic viral skin infections and HPV-driven malignancy.25 DOCK8 is also critical for actin cytoskeletal function and functions in a complex with WAS protein. Immune synapses are poorly formed in DOCK8-deficient cells, similar to WAS. Several distinct cellular defects in DOCK8-deficient patients that may underlie HPV-driven cancers include severe impairment of dendritic cell motility in skin, decreased numbers of plasmacytoid dendritic cells that fail to produce interferon α, and increased death of immune cells, including skin-resident CD8+ T cells, due to fragmentation while attempting to traverse through tissues (Figure 1).26
Common variable immunodeficiency
Patients with common variable immunodeficiency (CVID) have deficiency of antibody production and humoral immunity, with varying degrees of T-cell dysfunction and immune dysregulation (Figure 1). Because most patients with CVID are not genetically characterized, there is broad heterogeneity in disease manifestations. Lymphomas and lymphoproliferation are common, occurring in 17.2% of 1091 patients with CVID registered in the US Immunodeficiency Network.27 B-cell lymphopenia is common, and the additional replicative stress on B cells in the context of chronic inflammation is a likely contributor. In contrast to the distribution of B-cell lymphomas in otherwise healthy adults, there are few follicular lymphomas reported, skewing instead to extranodal marginal zone lymphoma and mucosa-associated lymphoid tissue lymphoma.28 Gastric cancers occur in patients with CVID more frequently than the general population and appear to be related to chronic inflammation and cell proliferation, possibly in conjunction with Helicobacter pylori infection. In an Italian registry of 455 patients with CVID, 25 patients had gastric cancer, with a standardized incidence ratio of 6.4, and this was the highest cause of death. The gastric cancers in the Italian series arose out of a background of atrophic gastritis, intestinal metaplasia, or dysplasia.29 Lymphoid and/or granulomatous infiltration of the gastrointestinal tract or lungs may further trigger excess immune cell proliferation. Although the incidence of malignant or proliferative disorders is clearly increased, routine surveillance is unlikely to be effective for early detection. Meticulous supportive care, maintaining a high degree of suspicion for malignancy, and aggressive workup of symptoms are key to managing patients with CVID.
Activated phosphoinositide 3-kinase-δ syndrome
A subset of patients previously diagnosed with CVID have been shown to harbor gain-of-function mutations in the genes encoding the catalytic subunit (p110δ) or biallelic loss-of-function mutations in the regulatory subunit (p85α) of the phosphoinositide 3-kinase-δ (PI3K-δ) protein. These mutations result in increased PI3K signaling in lymphocytes, where PI3K-δ is expressed.30 The fact that mutations in p110δ responsible for activated PI3K-δ syndrome (APDS) are present as somatic mutations in DLBCL, mantle cell lymphoma, and rarely Burkitt lymphoma supports a B-cell intrinsic role of overactive PI3K signaling in lymphomagenesis due to uncontrolled B-cell proliferation in the context of class switch recombination in germinal centers. These patients may have lymphoma, as in case 2, even before IEI is fully recognized. In addition, T cells in patients with APDS have impaired function and cytotoxicity, have exhausted CD8+ CD57+ T cells, and commonly develop T-cell lymphopenia and low naive T-cell counts over time (Figure 1).31
Ataxia-telangiectasia
Biallelic mutations in the autosomal gene ATM result in the syndrome of ataxia-telangiectasia, characterized by immunodeficiency, progressive cerebellar ataxia, oculocutaneous telangiectasia, and cancer predisposition.32 ATM is a kinase that has at least 2 critical roles in DNA repair. ATM is activated during double-stranded breaks generation (including during variable- diversity-joining region recombination) and recruits the MRE11/RAD51/NBS1 complex in a feed-forward cycle by phosphorylating histone H2AX. ATM-dependent phosphorylation of other targets mediates cell cycle arrest until DNA damage can be resolved. The broad function of ATM in DNA repair, within and outside of lymphocytes, results in multiple different cancers, including acute leukemia (both lymphoid and myeloid), Hodgkin lymphoma, NHL, and carcinomas (Figure 1).33 The degree of B-cell lymphopenia and antibody deficiency correlates with cancer risk.
GATA2 deficiency
Germline heterozygous mutations in the GATA2 gene, a transcription factor critical for HSC development and homeostasis, result in a wide variety of clinical manifestations, including atypical mycobacterial infection, DNA viral infections (herpes simplex virus, HPV, EBV, cytomegalovirus), lymphedema, bone marrow failure, myelodysplastic syndrome, and acute myeloid leukemia.34 GATA deficiency results in multiple cellular defects, including numerical deficiency of monocytes, dendritic cells, NK cells, and B cells; progressive stem cell loss; and accumulation of additional cytogenetic abnormalities such as monosomy 7 and trisomy 8. Whether the loss of mature immune cells is a manifestation of HSC loss vs cell intrinsic defects in survival or homeostasis is not clear. Here the immune defect per se, particularly the lack of NK cells, appears critical for the development of HPV-driven cancer.35 EBV+ lymphoma is far less common in GATA2 deficiency than EBV viremia and is related to immune defects including excess proliferation of B cells, poor dendritic cell number and function, and thereby poor T-cell response to EBV.36 The predisposition to myeloid leukemia in contrast is likely due to the parallel defect in hematopoiesis (Figure 1).
Principles of treatment of cancer in patients with IEIs
In general, patients with IEIs and cancer should undergo standard treatment, with the caveat that radiation-sensitive patients (eg, ataxia-telangiectasia) require dose modification or omission altogether of alkylating agents and radiation. Immunosuppressive agents such as corticosteroids, monoclonal antibodies that target B cells, fludarabine, and targeted inhibitors of JAK/STAT or BTK pathways further predispose to opportunistic infections. Additional antibiotic prophylaxis and scheduled replacement of immunoglobulins to maintain trough levels are critical components of supportive care.23
Correction of the underlying predisposing condition with allogeneic HSC transplantation consolidates cancer treatment and should be considered when feasible; it is the only avenue for long-term prevention of recurrence and definitive cure. The rapid rise in discovery of the genes responsible for IEIs has been paralleled by the development of gene therapy approaches, using integrating viral vectors to transduce autologous HSCs that are transplanted after appropriate conditioning.37 Gene therapy is an exciting alternative to allogeneic HSC transplant that obviates the need for a matched donor and avoids immunologic complications such as graft rejection and graft-versus-host disease altogether. Newer technologies based on gene editing also have promise.
Acknowledgments
This work was supported by funding from the Intramural Research Program, National Institutes of Health, National Cancer Institute, Center for Cancer Research. The authors acknowledge the contribution of Dr Ramya Ramaswami, who created Figure 2, and Dr Luigi Notarangelo, who provided case 2.
Conflict-of-interest disclosure
Sung-Yun Pai has no conflicts of interest to disclose and is supported by Center for Cancer Research, National Cancer Institute. Sung-Yun Pai's spouse is coinventor of a patent on combination therapies, including abiraterone to treat prostate cancer.
Kathryn Lurain receives research funding from Bristol Myers Squibb-Celgene Corporation, Merck, EMD Serono, Janssen Research, Lentigen Corp., CTI Biopharma and the National Cancer Institute.
Robert Yarchoan's research is funded in part by Cooperative Research and Development Agreements (CRADAs) between Celgene Corporation (now Bristol Myers Squibb, Co.) and the National Cancer Institute. He has also used drugs for his clinical and/or laboratory research provided to the NCI by Genentech Corp., Merck and Co., EMD Serono, Janssen Research, Lentigen Corp., and CTI Biopharma. Robert Yarchoan is a coinventor on patents on the treatment of KSHV-induced lymphoma using immunomodulatory compounds and uses of biomarkers, on peptide vaccines for HIV and other viral diseases, and on interleukin (IL)–12 as a treatment for Kaposi sarcoma. His spouse, who is also a US government employee, has patents on KSHV viral IL-6, analyzing single-cell epigenomes, inducing internalization of surface receptors, and vasostatin. It is his understanding that foreign patents have also been or will be filed for these inventions. These inventions were all made as full-time employees of the US government under 45 Code of Federal Regulations Part 7. All rights, title, and interest to these patents have been or should by law be assigned to the US Department of Health and Human Services. The government conveys a portion of the royalties it receives to its employee-inventors under the Federal Technology Transfer Act of 1986 (P.L. 99-502).
Off-label drug use
Sung-Yun Pai: Because most IEI present in childhood and very few drugs are formally approved for use in children, off-label drug use is discussed.
Kathryn Lurain: Off-label use of EPOCH for HIV-associated lymphomas and primary effusion lymphoma was discussed.
Robert Yarchoan: We broadly discuss the use of checkpoint inhibitors in PLWH but do not specify tumors for which they are FDA approved.
