Key Points
Administration of PROMs to adults with SCD VOCs is feasible and informative.
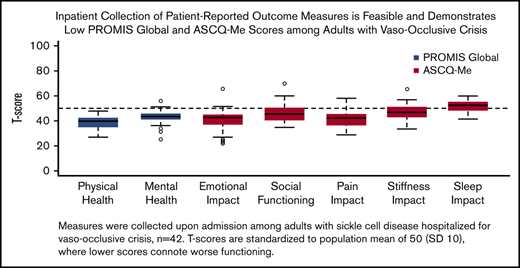
ASCQ-Me and PROMIS scores profiled the VOCs of hospitalized adults, showing poor health-related quality of life.

Abstract
Sickle cell disease (SCD) is characterized by painful vaso-occlusive crises (VOCs). Self-reported pain intensity is often assessed with the Numeric Rating Scale (NRS), whereas newer patient-reported outcome measures (PROMs) assess multidimensional pain in SCD. We describe pain experiences among hospitalized adults with VOCs, using 2 PROMs: the Patient-Reported Outcomes Measurement Information System (PROMIS) Global Health and the Adult Sickle Cell Quality of Life Measurement System (ASCQ-Me). Adults with SCD hospitalized with VOCs at 2 academic centers in Boston, Massachusetts, from April 2016 to October 2017 were eligible. Participants completed the NRS and PROMs at admission and 7 days postdischarge. PROM scores were described and compared with population norms. Length of stay (LOS) and 30-day readmission rates were assessed. Forty-two (96%) of 44 eligible patients consented and completed admission assessments. Mean age was 30.2 years (standard deviation, 9.1), 60% were women, 76% were non-Hispanic black, and 64% had hemoglobin SS. Twenty-seven participants (64%) completed postdischarge assessments. Sixty percent had ≥4 VOCs in the last year. Nearly all PROMIS Global Health and ASCQ-Me scores were worse than population norms. NRS and PROMIS Global Physical Health scores improved after discharge, the latter driven principally by improvements in pain. Overall median LOS was 7 days, and 30-day readmission rate was 40.5%. Administration of PROMs among adults with SCD hospitalized for VOCs is feasible and demonstrates participants experienced recurrent, prolonged, and severe VOCs. PROMIS Global and ASCQ-Me scores indicated substantial suffering, and the striking 30-day readmission rate highlights the vulnerability of these patients.
Introduction
Sickle cell disease (SCD) is a group of heritable hemoglobinopathies that represents the most prevalent blood disease in the United States, affecting >100 000 individuals.1,2 SCD is characterized by recurrent painful episodes, known as vaso-occlusive crises (VOCs), which are considered the hallmark of the disease.3-6 Although most patients with SCD manage their pain at home, and one-third of patients with SCD have no hospital or emergency department (ED) visits in a given year, VOCs are the leading cause of hospitalization.3,7-9
Despite the lack of a uniform definition of disease severity in SCD, an estimated 20% of adults with SCD age 18 to 30 years have ≥4 hospital admissions per year, constituting a subgroup more likely to have SCD-related complications and lower health-related quality of life (HRQL).10-13 This subgroup accounts for the most health care utilization, with frequent ED visits and hospital admissions.9-11,14,15 Furthermore, the Healthcare Utilization Project analysis of state inpatient databases found that patients with SCD and ≥4 hospitalizations annually accounted for 57% of all SCD-related hospital stays among Medicaid patients age 1 to 64 years.16 When adult patients with SCD are hospitalized with painful VOCs, all home-based therapies and supports have been exhausted, and hospital admission signals the need for escalated therapies.8,17
Clinical pain assessment in adults is most commonly performed with the Numeric Rating Scale (NRS), where individuals rate pain intensity from 0 (no pain) to 10 (worst imaginable pain).8,18,19 Because pain is inherently subjective and multidimensional, new tools for the measurement of the pain experience in SCD for use in outcomes research and clinical practice have been developed.20
The National Institutes of Health Patient-Reported Outcomes Information System (PROMIS) initiative has improved tools for clinical research with the development of measures to be used across the general population and among those with chronic illness, including SCD.21 Several of the PROMIS measures are generic and suitable for use across conditions and populations.22,23 For example, PROMIS Global Health is a generic measure of HRQL that generates separate Physical Health and Mental Health subscales. To date, PROMIS Global Health items have been shown to be predictive of key outcomes and future events, such as health care utilization and mortality.22,24
In contrast, disease-specific patient-reported outcome measures (PROMs) are used to evaluate disease impact among those with a particular health condition. To complement the generic instruments, the Adult Sickle Cell Quality of Life Measurement System (ASCQ-Me) was developed contemporaneously with PROMIS to assess the physical, social, and emotional impacts of SCD on adult functioning and wellbeing.25-27
ASCQ-Me has been validated in outpatient settings; PROMs are not routinely administered in inpatient settings because of concerns related to burden on patients and staff and potential threats to validity, including timing the assessments appropriately with respect to the measures’ recall periods, and ASCQ-Me has not been specifically validated during VOCs.27-29 Because SCD pain assessment is critical to disease management and HRQL among adults hospitalized with VOCs has yet to be described, we measured the VOC pain experience and its effect on HRQL and health care utilization among adults with SCD admitted with painful VOCs using both generic (PROMIS Global Health) and disease-specific measures of HRQL (ASCQ-Me).
Methods
Study design and participant characteristics
The study used an inception cohort of adults with SCD hospitalized with VOCs at Tufts Medical Center (Tufts MC) and Boston Medical Center (BMC) from April 2016 to October 2017. Adults age ≥18 years with SCD (genotypes hemoglobin [Hb] SS, Hb SC, Hb Sβ+ thalassemia, Hb Sβ0 thalassemia, and other/unspecified) admitted to Tufts MC or BMC inpatient services with VOCs were eligible. Patients were ineligible if they were unable to provide written informed consent or were non-English speaking, because ASCQ-Me was only available in English during this study period.
Study measures
Self-reported sociodemographic and medical history information included age, sex, insurance, education, living situation, dependency status, employment, disability, disease genotype, and hydroxyurea prescription. Patients reported pain intensity on the 11-point NRS, where a 1-point change is considered a minimal clinically important difference.8,18,19,30
The PROMIS Short-Form (version 1.1) Global Health scale is a generic measure of HRQL that assesses physical, mental, and social health. It has a recall period of 7 days and yields separate Physical Health and Mental Health subscale scores, which range from 0 to 100 and are standardized to a US population mean of 50 and standard deviation (SD) of 10.22,23 For each subscale, a higher score connotes better functioning, and a 3- to 5-point (SD, 0.3-0.5) change is considered clinically meaningful.22,30-35
ASCQ-Me is an SCD-specific PROM that begins with the 5-item Pain Episode scale, which assesses frequency, timing, and severity of sickle cell pain events, serving as an indicator of SCD severity over the prior year. The Pain Episode scale generates separate Frequency and Severity subscale scores that range from 0 to 100 and are standardized to an SCD population mean of 50 (SD, 10).25-27,31,32,36,37 In contrast to the other PROMIS and ASCQ-Me scales, higher scores on the Pain Episode subscales connote worse impact, with more frequent and more severe disease, respectively.26,36
The remainder of ASCQ-Me is composed of 5 short forms, each with 5 items that assess the impacts of SCD: Emotional Impact, Social Functioning Impact, Pain Impact, Stiffness Impact, and Sleep Impact.27,37 Emotional Impact assesses feelings of worry, depression, and loneliness; Social Functioning Impact assesses general activities and activities with family and friends; Pain Impact assesses pain severity and interference with functioning; Sleep Impact assesses getting to sleep, staying asleep, falling back asleep, and getting enough sleep; and Stiffness Impact assesses general stiffness, joint stiffness, and interference with movement.25,26,37
The ASCQ-Me recall period is 7 days, except for Social Functioning Impact, which has a 30-day recall period. Scores for ASCQ-Me scales range from 0 to 100, with a standardized SCD population mean of 50 (SD, 10), where lower scores connote worse disease impact.26,31,36,37 Because there is currently no published minimal clinically important difference for the ASCQ-Me measures, we assumed a minimal clinically important difference to be a 3- to 5-point (SD, 0.3-0.5) change, similar to PROMIS scores.33-35 During our study, the ASCQ-Me Medical History Checklist was not publicly available.
Health care utilization outcomes included hospital length of stay (LOS) in days and 30-day hospital readmission rate to Tufts MC or BMC, collected from the electronic health record.
Study procedures
Participants provided sociodemographic and medical history information upon hospital admission for VOCs, at which time the ASCQ-Me Pain Episode measure (Frequency and Severity subscales) was also completed. Because participants were expected to have varying LOSs, PROMIS Global Health and the remainder of ASCQ-Me were collected on admission and 7 days postdischarge (within 2-day window). ASCQ-Me Social Functioning Impact was not analyzed in the 7-day postdischarge assessment, because its 30-day recall period would overlap with the admission assessments. In the event of hospital readmission within 1 week, PROMIS Global Health and ASCQ-Me were not collected for the 7-day postdischarge assessment.
The NRS is part of usual standard care and was abstracted upon admission from the electronic health record for each participant. The NRS was also collected 7 days postdischarge.
All assessments at the time of hospital admission were collected with pen and paper, and assessments after discharge were collected via telephone report by a trained researcher (K.S.E.). If participants did not respond to the first telephone call at 7 days postdischarge, participants were phoned once daily for 2 days for a maximum of 3 telephone calls.
Statistical analysis
Descriptive statistics were used to describe feasibility of PROM collection at the time of hospital admission and 7 days postdischarge. Means and frequencies of sociodemographic and SCD characteristics among the study sample were reported.
ASCQ-Me Pain Episode Frequency and Severity subscale scores were reported and compared using a 1-sample Student t test with the outpatient ASCQ-Me validation sample scores of 561 participants (50; SD, 10), the reference population for ASCQ-Me.26,27 Pain Episode item 2 (“When was your last pain attack [crisis]?”) responses were all coded as “I have one right now.”26
Summary statistics with means and SDs were reported for scales at admission and 7 days postdischarge for the overall cohort. Mean PROMIS Global Health and ASCQ-Me scores at admission and 7 days postdischarge were compared using a 1-sample Student t test with general (50; SD, 10) and SCD-specific population norms (50; SD, 10), respectively. Using a 1-sample Student t test, change scores (7-day postdischarge score minus admission score) for PROMIS and ASCQ-Me Emotional Functioning, Pain, Stiffness, and Sleep Impact measures were compared with 0 among complete cases, where participants missing 7-day postdischarge assessments were excluded. Characteristics and admission PROM scores of participants who completed the 7-day postdischarge assessment were compared with those of participants who did not, using a χ2 or Fisher’s exact test for categorical variables and a 2-sample Student t test for age, NRS, and PROM scores.
Because the PROMIS Global Physical Health subscale score includes 1 item that uses average 0-to-10 pain score over the past 7 days (Global 07), which is similar to the NRS, the individual PROMIS Global Physical Health item change scores were compared with 0 using a 1-sample Student t test.
Known-group validity assesses the degree to which measures are able to distinguish differences between groups that are known to be different.28 Known-group comparisons by VOC frequency, an indication of disease severity, were performed on the basis of response to the number of self-reported VOCs during the preceding year (ASCQ-Me Pain Episode item 1). This disease severity criterion was selected because prior studies have demonstrated that young adults with SCD who have ≥4 hospitalizations per year are more likely to have SCD-related complications, have lower HRQL, and account for the most health care utilization.9-16 High- and low-frequency groups were categorized as ≥4 and <4 VOCs in the prior year, respectively. Summary statistics with means and SDs were reported by scale at admission among the VOC high- and low-frequency groups. Characteristics and admission PROM scores of VOC high- and low-frequency groups were compared with a χ2 or Fisher’s exact test for categorical variables and a 2-sample Student t test for age, NRS, and PROM scores. Summary statistics for hospital LOSs and 30-day readmission rates were also calculated.
Study data were collected and managed using Research Electronic Data Capture, a secure, Web-based application for electronic data capture hosted at Tufts MC.38 The study protocol was approved by the Tufts Health Sciences Institutional Review Board at Tufts MC. The study was approved by BMC and the Boston University Medical Campus Institutional Review Board with a data-sharing agreement. All statistical analyses were performed at Tufts MC using R statistical software (version 3.4.2; RStudio version 1.1.383; www.r-project.org) and a 2-sided α of 0.05.
Results
Sociodemographic and SCD characteristics
Of 44 eligible participants, 42 enrolled (Figure 1). Two participants declined, citing reasons of psychological distress and fatigue. All enrolled participants completed the admission assessments. However, only 27 (64%) completed 7-day postdischarge assessments. Missingness was meaningful; nearly half were due to hospital readmissions (n = 7). The remainder were nonrespondent at 7 days postdischarge (n = 8).
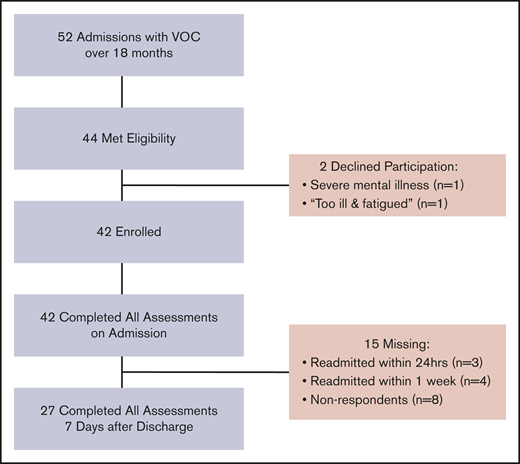
Flow diagram of study participants. Depiction of patient participation upon hospital admission with VOCs. At time of hospital admission, participants provided sociodemographic and disease characteristics. Participants then completed the admission pain assessment consisting of NRS collected from the electronic health record and PROMIS Global Health and ASCQ-Me measures. Seven days after hospital discharge, participants completed NRS, PROMIS Global Health, and ASCQ-Me assessments via telephone report.
Flow diagram of study participants. Depiction of patient participation upon hospital admission with VOCs. At time of hospital admission, participants provided sociodemographic and disease characteristics. Participants then completed the admission pain assessment consisting of NRS collected from the electronic health record and PROMIS Global Health and ASCQ-Me measures. Seven days after hospital discharge, participants completed NRS, PROMIS Global Health, and ASCQ-Me assessments via telephone report.
Mean age was 30.2 years (SD, 9.1; range, 18-61), 60% were women, and there was a predominance of Hb SS genotype, consistent with more clinically severe disease manifestation (Table 1). All patients were insured, and 88% had public insurance. Sixty percent reported being on disability, and one-third had achieved a high school or lower level of education.
Admission ASCQ-Me Pain Episode
Admission ASCQ-Me Pain Episode scores demonstrated more frequent and more severe VOCs in this hospitalized sample as compared with the outpatient validation sample.27 Mean ASCQ-Me Pain Episode Frequency score was 60.4 (SD, 4.2) and Severity score was 55.7 (SD, 6.6), both of which were significantly higher than the validation sample mean of 50 (P < .001), reflecting worse VOC episodes.
Admission and 7-day postdischarge NRS, PROMIS Global Health, and ASCQ-Me profiles
There were no statistically significant differences in mean age, sex, Hb SS genotype, hydroxyurea prescription, public insurance status, disability status, educational level, or mean PROM scores (NRS, PROMIS Global Health, ASCQ-Me) between those who completed the 7-day postdischarge assessment and those who did not (results not shown). However, participants who completed the postdischarge assessment were more likely to be non-Hispanic black (89% vs 53%; P = .02) and less likely to have dependent children at home (11% vs 40%; P = .049).
Mean NRS on admission was 8.4 (SD, 1.9), signifying severe pain intensity among study participants (Table 2). There was statistically significant and clinically meaningful improvement in mean NRS pain score, from 8.5 (SD, 2.1) to 5.6 (SD, 3.1), with a change score of −2.9 (SD, 4.2), by 7 days postdischarge among the 27 respondents with complete follow-up (P = .001; Table 2).
Mean PROMIS Global Physical Health subscale scores were more than a full SD below the US population mean upon admission (38.9; SD, 5.0; P < .001) and 7 days postdischarge among respondents (40.9; SD, 4.7; P < .001); change scores reached borderline statistically significant improvement among those with complete follow-up (2.2; SD, 5.5; P = .05; Table 2). This change in PROMIS Global Physical Health was primarily driven by clinically meaningful and statistically significant improvement in mean 0-to-10 pain score (item Global 07; mean change, −1.0 points; SD, 1.1; P = .002), whereas change scores for the other PROMIS Global Physical Health items were not significant (results not shown). Mean PROMIS Global Mental Health subscale scores were significantly below US population norms on admission (42.2; SD, 6.0; P < .001) and 7 days postdischarge (44.7; SD, 5.8; P < .001); however, the PROMIS Global Mental Health change scores were not statistically significant among those with complete follow-up (Table 2).
Admission and 7-day postdischarge scores on ASCQ-Me Emotional Impact, Social Functioning Impact, and Pain Impact, as well as 7-day postdischarge Stiffness Impact, were significantly below SCD-specific population norms. Emotional Impact scores were a full SD below the population mean at both admission (40.5; SD, 9.1) and 7 days postdischarge (40.8; SD, 7.5). None of the ASCQ-Me change scores were statistically significant (Table 2).
Known-group comparisons by VOC frequency
Sixty percent of study participants reported ≥4 pain crises in the prior year, constituting the VOC high-frequency group. Although participants with high VOC frequency tended to be younger and of non-Hispanic black race, have Hb SS genotype, have been prescribed hydroxyurea, and be on disability, as compared with the VOC low-frequency group, only disability status was statistically significant (P = .02; Table 3).
Known-group comparison by VOC frequency in the prior year demonstrated that participants in the VOC low-frequency group had significantly worse PROMIS Global Mental Health subscale scores on admission (39.4; SD, 6.2) as compared with the VOC high-frequency group (44.2; SD, 5.2; P = .01; Table 3). Although the high-frequency group tended to have, on average, lower ASCQ-Me scores on admission, these results were not statistically significant.
Health care utilization
Median LOS in the study cohort was 7 days (range, 1-44; mean, 8.5; SD, 8.1), and the 30-day rate of hospital readmission was 40.5%. Of the hospital readmissions within 30 days, 18% occurred within 24 hours, 29% occurred within 1 week, and the remaining 53% occurred between 1 and 4 weeks.
Discussion
PROMIS Global Health and ASCQ-Me scores profile the multidimensional pain experience of adults with SCD admitted with VOCs. We demonstrate the acceptability and feasibility of collecting PROMs in the inpatient setting from adults with SCD despite the intensity and severity of participants’ clinical status at the time of hospital admission. Admission ASCQ-Me Pain Episode scores reflected recurrent, prolonged, and severe VOC episodes over the prior year. Most generic and disease-specific scores as measured by PROMIS Global Health and ASCQ-Me were well below population norms on admission and at 7 days postdischarge, with the exceptions of Stiffness Impact on admission and Sleep Impact at admission and 7 days postdischarge. These findings are indicative of ongoing substantial suffering from the VOC pain experience as compared with the general US population and with outpatients with SCD.
Concerns regarding the relevance of Pain Episode item 2 (“When was your last pain attack [crisis]?”) at the time of an acute VOC were raised because several respondents requested clarification regarding whether to respond based on the current VOC or the “last pain attack [crisis],” despite 1 of the response choices stating “I have one right now.” Because all participants were admitted with VOCs, we reassigned 13 participants to “I am having one now.” This allowed us to compare of the Pain Episode Frequency Subscale score from our study with those of the ASCQ-Me reference population.26,27 Future researchers using this scale during acute VOCs should be aware of this area of potential confusion.
Although pain intensity (NRS) and PROMIS Global Physical Health improved 7 days postdischarge, other HRQL scale scores did not. It is likely that resolution of the VOC was incomplete in the 1 week after hospital discharge for all participants. Moreover, although acute pain (eg, NRS) and its impact on overall physical functioning may improve, some domains may not recover after an acute VOC. For instance, worsening of the ASCQ-Me Stiffness Impact score 7 days postdischarge, although a small, not statistically significant change, suggests that some patients may either worsen or have increased mobility and thus more opportunity to experience stiffness after hospital discharge. PROMIS Global Mental Health and ASCQ-Me Emotional Impact scores remained low, supporting the need to assess the impact of the pain experience on individuals with SCD above and beyond the current standard of pain intensity to identify other areas in need of clinical attention.
Participants with low VOC frequency had worse mental health scores as measured by PROMIS Global Mental Health, as compared with the VOC high-frequency group. Further study of this finding is needed. Although this may be counterintuitive, one hypothesis is that mental health is more severely affected at the time of hospital admission by the sudden and disruptive occurrence of an acute VOC among individuals who are infrequently affected by pain crises. One could speculate that mental health scores among individuals with infrequent crises would be better than those who have frequent crises, if assessed at times outside of an acute VOC. Another explanation is that because our overall sample reported frequent and severe VOCs, they may represent a generally more severe group such that there was a lack of detectable difference between known groups on the ASCQ-Me scales. Self-reported VOC frequency may not be equivalent to the number of VOCs requiring hospitalization, which may have contributed to these negative findings. This is supported by recent evaluation of ASCQ-Me among 224 adult outpatients with SCD in the United Kingdom, where patients with ≥3 hospitalizations in the prior year were indeed found to have poorer HRQL on all ASCQ-Me scales as compared with those less frequently admitted.28
Compared with analyses from the Healthcare Utilization Project, mean LOS in the study cohort was 8.5 days (median, 7; range, 1-44) vs 5.5 days, and the 30-day rate of hospital readmission was 40.5% in the study cohort vs 41.1% (among adults age 18-30 years).9,39
The lengthy hospital stays and strikingly high 30-day readmission rate highlight that adult SCD patients hospitalized with VOCs are a particularly vulnerable population. Prior research has shown that the readmission rate is highest among those age 18 to 30 years and decreases with advancing age.9 In an analysis from the Bethesda Sickle Cell Cohort Study, among 264 adults with Hb SS disease, the self-reported number of severe VOCs over the prior year was shown to be a relevant measure of both severity of SCD and risk of death.11 Furthermore, frequent hospitalizations have been shown to be predictive of early mortality, and hospital readmission within 1 week of discharge was associated with death.40,41
Assessing the pain experience from the perspective of patients with SCD with a brief and comprehensive assessment is critical to our enhanced understanding of the pain experience and its impact on those living with SCD. Use of PROMs is an important step toward advocacy for adults with SCD to help address the stigmatization associated with SCD and to give voice to the experience of pain and the impact of VOCs on wellbeing and HRQL in a standardized fashion.42-44 In 2014, the National Institutes of Health guidelines for the management of SCD supported listening to the patient’s voice regarding his or her pain experience to guide pain mitigation.45 Furthermore, there is growing evidence that PROMs improve communication between patients and providers, and a recent seminal randomized controlled trial showed PROM implementation improved survival among patients with advanced malignancies receiving usual cancer treatment.42,46-50
In this study, we demonstrate that prospective, longitudinal collection of these novel yet preliminarily validated PROMs is feasible and informative in an inpatient setting, enriching our understanding of the individual pain experience among adults with SCD admitted with pain from an acute VOC, as informed by self-reported measures of PROMIS Global Health and ASCQ-Me. This assessment is brief and sufficiently comprehensive to capture the pain experience of an acute VOC and the multidimensional impact on wellbeing and functioning.
Future studies of the responsiveness of PROMIS Global Health and ASCQ-Me measures to changes in the pain experience over time should take into consideration the duration and time to recovery from VOCs, the high readmission rate within 7 days postdischarge, and the potential for individuals to experience decrements in HRQL with each VOC, reflective of the accumulation of end-organ damage. Future research pertaining to the validity of the ASCQ-Me Medical History Checklist as a measure of SCD severity is needed, particularly because there is no standard definition of SCD severity to date.
This study has several strengths, including adding to the evidence supporting validity of ASCQ-Me and demonstration of feasibility of administering PROMs to an inpatient sample experiencing acute VOCs, a population previously not studied or validated as part of the initial development of ASCQ-Me. However, we acknowledge the study’s limitations. Results may not be generalizable to the entire US population of adults with SCD, because only adults hospitalized for VOC-associated pain, indicative of more severe manifestations of SCD, were included. In addition, the lack of a national registry of patients with SCD prevents comparisons of the study sample with the larger population on factors such as disability and employment, living situation, and hydroxyurea. However, consistent with available data, ∼60% of study participants had Hb SS followed by Hb SC, with most individuals identifying as non-Hispanic black.1 Similar to prior studies, most participants were young adults and publicly insured.16,39 Adult women may have been overrepresented in the current sample (59.5%), although this sex difference in study participation is consistent with prior studies.25,26,51,52 There is potential for bias on assessments collected by telephone, where participants may have responded to the interviewer in a more favorable manner.29 However, there is generally high reliability of PROMIS measures across modes of administration, although ASCQ-Me has not been studied outside of self-report.29,37,53,54
Although a participant could have been readmitted to a nonstudy site hospital and thus not captured, our 30-day readmission rate is comparable to prior research, suggesting this was not a major limitation.9 We encountered nonignorable missing data at 7 days postdischarge, primarily resulting from hospital readmissions, which limits interpretability of change scores because the complete cases are likely not representative of more medically ill participants who required readmission. Future studies with larger sample sizes may employ pattern-mixture modeling conditioned on the reason for missingness or multiple imputation to analytically address missing data.55 We also acknowledge the challenges of interpreting change scores (from admission to 7 days postdischarge), because the initial assessment was done at the time of an acute VOC and did not constitute baseline functioning. Moreover, because not all participants completed the 7-day postdischarge assessment, power was limited to detect changes in scores. Nevertheless, changes in NRS and Pain Impact approached the minimally important clinical difference.
In conclusion, this study deepens our understanding of the assessment of pain among adults with SCD above and beyond the current standard of 0-to-10 pain intensity through the use of PROMs. In this study, adults with SCD hospitalized with painful VOCs had recurrent, prolonged VOCs over the prior year with associated severe impairments across most HRQL domains as measured by PROMIS Global Health and ASCQ-Me both upon hospital admission and 7 days after discharge, thereby adding to the evidence establishing validity of these PROMs.
Acknowledgments
This study was funded in part by the Komen for the Cure Graduate Training in Health Disparities Grant (K. Freund and S.K.P., dual principal investigators; K.S.E., Komen Scholar) and by the National Center for Advancing Translational Sciences, National Institutes of Health, award UL1TR002544.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Authorship
Contribution: K.S.E. conceptualized the study, curated the data, designed the methods, administered the study, performed the statistical analysis, made the tables and figure, and wrote and edited the paper; A.M.R. and F.N. contributed to the methodology, supervised the statistical analyses, and reviewed and edited the paper; H.P.S. and R.J.B. contributed to the study design and reviewed and edited the paper; R.A.W. provided project administration support and reviewed and edited the paper; and S.K.P. acquired funding support, provided resources, and supervised all aspects of the project, including data validation and manuscript writing and editing.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
The current affiliation for K.S.E. is Division of Hematology, University of Washington, Seattle, WA.
The current affiliation for H.P.S. is Medstar Washington Hospital Center, Washington, DC.
The current affiliation for F.N. is Bouvé College of Health Sciences, Northeastern University, Boston, MA.
Correspondence: Kimberly S. Esham, Division of Hematology, University of Washington, 1705 NE Pacific St, Box 357710, Seattle, WA 98195; e-mail: kimesham@uw.edu; and Susan K. Parsons, Tufts Medical Center Institute for Clinical Research and Health Policy Studies, 800 Washington St, Box 345, Boston, MA 02111; e-mail: sparsons@tuftsmedicalcenter.org.