

Key Points
IUT enables rapid immune reconstitution and avoids many clinical and economic problems; however, the indication is still limited.
IUT may be a treatment option in select cases, eg, fetuses exposed to a significant infectious risk, where a matched sibling donor exists.
Introduction
X-linked severe combined immunodeficiency (SCID-X1) is a rare disorder caused by defects in the IL2RG gene coding for the common γ chain (a cytokine receptor subunit common to at least 6 different interleukin receptors). The standard treatment of SCID-X1 is allogeneic hematopoietic stem cell transplantation (HSCT).
Here, we report on a successful in utero transplantation (IUT) in a SCID-X1 fetus via the ultrasound-guided intravascular infusion of hematopoietic stem cells (HSCs) into the umbilical vein. The patient (36 months old at the time of writing) is the third child of a woman carrying an IL2RG mutation. Prenatal tests (performed at gestational week 10 because of the fetus’ male sex) predicted a T−B+ SCID caused by a hemizygous c.697delA mutation (p.Ser233ValfsX40). The patient’s 4-year-old sister was found to be HLA matched, and postnatal HSCT was scheduled. At a standard serologic screening visit at the end of the first trimester of pregnancy, the mother was diagnosed with a primary Toxoplasma gondii infection. The decision to perform IUT was taken to avoid the potentially serious consequences of late maternofetal transmission of Toxoplasma.1 After the provision of the parents’ written, informed consent and approval by the French regulatory authorities, bone marrow–derived HSCs were harvested. Immunoselected CD34+ cells (15 × 106) and a preparation of CD34− cells containing 8 × 106 T lymphocytes were infused into the umbilical vein at gestational week 25. The result of a polymerase chain reaction (PCR) assay for toxoplasmosis in the amniotic fluid was negative. In line with current French guidelines, the mother was treated with spiramycin until delivery.
Methods
Prenatal genetic testing (targeted Sanger sequencing of IL2RG exon 5 and flanking microsatellites study) was performed on genomic DNA extracted from a chorionic villus sample. Signal-joint and β-chain T-cell receptor excision circles (TRECs) were quantified using a real-time quantitative PCR assay, as described previously.2 Chimerism was studied using (1) fluorescence in situ hybridization and X- and Y-chromosome–specific probes according to the manufacturer’s protocol (Cytocell, Cambridge, United Kingdom) and (2) real-time quantitative PCR assays for donor- and recipient-specific single-nucleotide polymorphisms (KMRtype and KMRtrack chimerism monitoring reagents; GenDx).3 The T-cell receptor γ repertoire was assessed using single-tube, EuroClonality-inspired multiplex PCR, as described elsewhere.4,5 The IUT was performed by ultrasound-guided infusion into the umbilical vein.6
Prior the in utero engraftment, the procedure was approved by the French Competent Authority, investigators have complied with the applicable regulatory requirements and the ethical principles that have their origin in the Declaration of Helsinki. They provided a documented patient information sheet to the family, and informed consent was duly signed prior to engraftment. The investigators received an institutional review board’s favorable opinion of the written informed consent form.
Please see supplemental Methods for a more detailed description of the methods used.
Results and discussion
No adverse events were observed during or after the cell infusion. The course of pregnancy was uneventful, and a healthy baby (birth weight, 3930 g; height, 52 cm; head circumference, 36 cm) was born at term.
Peripheral blood samples were analyzed at birth and at several time points thereafter as part of our routine posttransplant care. Immune reconstitution was tracked over time (Figure 1; Table 1). A high proportion of CD4+ cells coexpressed the CD45RA antigen, suggesting the presence of effective de novo thymopoiesis (Figure 1; Table 1). The cord blood predominantly contained naive T cells (CCR7+CD45RA+CD45RO−) with a memory stem cell phenotype (CD95+) (Table 1; supplemental Figure 1). It is noteworthy that the low TREC level at birth increased gradually over time (Figure 1). The β-chain TREC level and intrathymic proliferation were similar to those observed in healthy infant donors (<4.5 years of age) in our establishment, suggesting that posttransplantation thymopoiesis was normal.
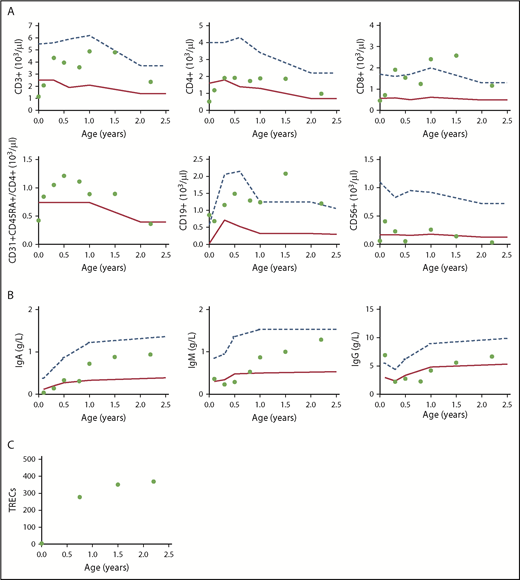
Immune reconstitution after birth. (A) CD3+, CD4+, CD8+, CD31+CD45RA+CD4+, CD19+, and CD56+ cell counts. (B) Immunoglobulin A (IgA), IgM, and IgG reconstitution. (C) TRECs. Dots correspond to the values recorded. The lower and upper boundaries of the age-specific normal range are indicated by solid and dashed lines, respectively.
Immune reconstitution after birth. (A) CD3+, CD4+, CD8+, CD31+CD45RA+CD4+, CD19+, and CD56+ cell counts. (B) Immunoglobulin A (IgA), IgM, and IgG reconstitution. (C) TRECs. Dots correspond to the values recorded. The lower and upper boundaries of the age-specific normal range are indicated by solid and dashed lines, respectively.
Hematopoietic and immune reconstitution in the peripheral blood after birth
| At birth | 3 wk | 3 mo | Age-matched reference values (for <6 mo) | 6 mo | 12 mo | 19 mo | 27 mo | Age-matched reference values (for last follow-up) | |
|---|---|---|---|---|---|---|---|---|---|
| Hemoglobin, g/dL | 16.6 | 12.8 | 10.9 | 10-14 | 10.5 | 11.4 | 12.5 | 11.5 | 11.5-13.5 |
| Platelets, × 109/L | 293 | 452 | 671 | 175-500 | 485 | 403 | 414 | 261 | 175-500 |
| Neutrophils, × 109/L | — | 5.7 | 4.2 | 1.0-9.0 | 2.5 | 1.9 | — | 2 | 1.5-8.5 |
| Lymphocytes, × 109/L | 2.1 | 3.4 | 5.8 | 2-13.5 | 5.5 | 6.4 | 7.2 | 3.6 | 3-9.5 |
| CD3+, % | 55 | 61 | 75 | 53-84 | 72 | 75 | 67 | 65 | 56-75 |
| CD4+, % | 25 | 35 | 33 | 35-64 | 35 | 29 | 26 | 27 | 28-47 |
| CD8+, % | 22 | 21 | 33 | 12-28 | 28 | 37 | 36 | 32 | 16-30 |
| CD4+CD45RA+, % | 96 | 89 | 75 | 88-95 | 85 | 96 | 72 | 52 | 73-86 |
| CD31+CD45RA+CD4+, % | 81 | 71 | 55 | 60-72 | 63 | 47 | 48 | 37 | 57-65 |
| CD4+CCR7+CD95+, % | 87 | — | 14.3 | NA | — | — | — | — | NA |
| CD8+CCR7+CD95+, % | 90 | — | 3.46 | NA | — | — | — | — | NA |
| CD19+, % | 41 | 20 | 20 | 6-32 | 27 | 19 | 29 | 33 | 7.6-28.2 |
| CD16+CD56+, % | 3 | 12 | 4 | 4-18 | 1 | 4 | 2 | 1 | 4-17 |
| PHA T-cell proliferation, CPM/103 | 21.5 | — | — | >50 | 136 | 65 | 48 | — | >50 |
| Tetanus toxoid T-cell proliferation, CPM/103 | — | — | — | >10 | — | 5.8 | 72 | — | >10 |
| At birth | 3 wk | 3 mo | Age-matched reference values (for <6 mo) | 6 mo | 12 mo | 19 mo | 27 mo | Age-matched reference values (for last follow-up) | |
|---|---|---|---|---|---|---|---|---|---|
| Hemoglobin, g/dL | 16.6 | 12.8 | 10.9 | 10-14 | 10.5 | 11.4 | 12.5 | 11.5 | 11.5-13.5 |
| Platelets, × 109/L | 293 | 452 | 671 | 175-500 | 485 | 403 | 414 | 261 | 175-500 |
| Neutrophils, × 109/L | — | 5.7 | 4.2 | 1.0-9.0 | 2.5 | 1.9 | — | 2 | 1.5-8.5 |
| Lymphocytes, × 109/L | 2.1 | 3.4 | 5.8 | 2-13.5 | 5.5 | 6.4 | 7.2 | 3.6 | 3-9.5 |
| CD3+, % | 55 | 61 | 75 | 53-84 | 72 | 75 | 67 | 65 | 56-75 |
| CD4+, % | 25 | 35 | 33 | 35-64 | 35 | 29 | 26 | 27 | 28-47 |
| CD8+, % | 22 | 21 | 33 | 12-28 | 28 | 37 | 36 | 32 | 16-30 |
| CD4+CD45RA+, % | 96 | 89 | 75 | 88-95 | 85 | 96 | 72 | 52 | 73-86 |
| CD31+CD45RA+CD4+, % | 81 | 71 | 55 | 60-72 | 63 | 47 | 48 | 37 | 57-65 |
| CD4+CCR7+CD95+, % | 87 | — | 14.3 | NA | — | — | — | — | NA |
| CD8+CCR7+CD95+, % | 90 | — | 3.46 | NA | — | — | — | — | NA |
| CD19+, % | 41 | 20 | 20 | 6-32 | 27 | 19 | 29 | 33 | 7.6-28.2 |
| CD16+CD56+, % | 3 | 12 | 4 | 4-18 | 1 | 4 | 2 | 1 | 4-17 |
| PHA T-cell proliferation, CPM/103 | 21.5 | — | — | >50 | 136 | 65 | 48 | — | >50 |
| Tetanus toxoid T-cell proliferation, CPM/103 | — | — | — | >10 | — | 5.8 | 72 | — | >10 |
CPM, counts per minute; NA, not available; PHA, phytohemagglutinin.
The postnatal clinical course was uneventful, and the baby was discharged 5 days after birth. No restrictions were placed on the baby’s everyday life, and he was breastfed. The presence of normal neutrophil, hemoglobin, and platelet counts from birth onwards testified to a normal hematopoiesis (Table 1). The patient did not require red blood cell or platelet transfusions.
The circulating T lymphocyte count rose steadily, and the subset counts normalized between 1 and 3 months after birth. The memory T-cell count and TREC level increased progressively, in line with exposure to the environment and as immune reconstitution continued (Figure 1; Table 1). In vitro lymphoproliferative responses to common T-cell mitogens and alloantigens normalized by 6 and 19 months, respectively (Table 1). A polyclonal T-cell receptor γ repertoire was observed at 12 months (supplemental Figure 2). Congenital toxoplasmosis was ruled out by negative serologic assay results.
The B-cell count was normal from birth onwards. Immunoglobulin production increased over time and had normalized by month 6 (Figure 1). An assessment of the B-cell subset distribution at last follow-up showed the presence of CD27+IgD− switched memory B cells and CD27+IgD+ marginal zone B cells, although the proportions (1% and 2% of the CD19+ cells, respectively) were lower than age-matched reference values. Postvaccination antibody titers measured several months after immunization were normal for diphtheria and tetanus and partially positive for Pneumococcus antigens (supplemental Table 1). Immunoglobulin replacement therapy was not required at any time, and a normal subset of follicular helper T cells was observed (supplemental Figure 3). In order to determine the origin of the patient’s circulating B cells, we characterized the donor-recipient chimerism in sorted blood subpopulations. The T cells proved to be donor derived, while the circulating B cells, monocytes, and neutrophils were recipient derived (supplemental Table 2).
At present, the patient is healthy; no signs of graft-versus-host-disease have been detected, and hospitalization has never been required.
Here, we report a successful IUT in a fetus with SCID-X1. Transplantation led to sustained, protective immune reconstitution soon after birth and yielded normal numbers of functional circulating T cells with a polyclonal repertoire. We observed that memory stem cells were prevalent at birth; the low TREC levels in these cells7 might explain why the initially low value rose progressively in parallel with T-cell recovery, demonstrating effective thymopoiesis. This finding is in line with the dynamic thymopoiesis observed after early postnatal HSCT in SCID (evidencing normal thymic function in the complete absence of infections) and reports in which HSCT early in life leads to a higher thymic output and a higher survival rate.8 The low observed natural killer cell count was similar to that obtained after HSCT in the absence of conditioning. Post-IUT B-cell reconstitution in SCID is still subject to debate.9 Interestingly, our patient displayed normal immunoglobulin levels and did not require immunoglobulin replacement therapy, although the circulating B cells were recipient derived.
As reported in the literature, IUT has several potential advantages; it avoids the problems associated with postnatal transplantation and may induce donor-specific tolerance.10-13 However, clinical experience with IUT is limited by the lack of sustained donor engraftment and the risks associated with the procedure. The best results have been obtained in SCID-X1, thanks to the healthy cells’ large selective advantage. In the present case, an HLA-identical donor was available; most of the IUTs reported in the literature are haploidentical transplants, which are more complex and may have a less satisfactory outcome.12 In IUT, donor cells can be infused into the peritoneum or umbilical vein; the latter procedure is much more efficient but more technically demanding.
As suggested elsewhere, IUT is a potential treatment for certain congenital disorders.13 Furthermore, IUT could be usefully combined with more specific, less toxic conditioning methods, such as the antibody-mediated depletion of recipient HSCs.14,15
In conclusion, IUT via ultrasound-guided cell infusion was safe. It enabled rapid immune reconstitution and avoided many clinical and health economic problems. However, the risks associated with the procedure and the high success rate achieved by early postnatal transplantation limit the indication for IUT. Nevertheless, this procedure may be a treatment option in selected cases, such as fetuses exposed to a significant risk of infectious disease.
The full-text version of this article contains a data supplement.
Acknowledgments
The authors acknowledge the patient and his family and thank Amélie Trinquand and Loic Chentout for excellent technical assistance. S.K. is a staff researcher at the Centre National de la Recherche Scientifique.
Authorship
Contribution: M.C., S.B., J.-M.J., C.P., and A.M. provided family care and follow-up, designed the study, and collected and analyzed the data; J.-M.J., M.C., S.B., A.-M.D., A.M., E.M., B.T., and J.N. prepared and performed the transplantation; C.P. and J.R. performed prenatal genetic diagnoses; C.P., J.R., M.C., A.M., F.T., A.G., C.R., and S.K. performed immunological assessments; A.M. and M.C. wrote the paper; A.M., M.C., C.P., S.B., J.-M.J., J.R., F.T., S.K., N.M., A.T., E.C., E.M., and I.R.-W. critically reviewed the manuscript; A.T. and E.C. performed the TREC analysis; E.M., M.A., and I.R.W. performed the chimerism analysis; and N.M. and L.C. provided clinical data and technical support.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Alessandra Magnani, Biotherapy Department, Necker-Enfants Malades University Hospital, 149 Rue de Sèvres, 75015 Paris, France; e-mail: alessandra.magnani@aphp.fr.

