

Key Points
TA-TMA involves the CNS, is underdiagnosed, and should be included in the differential diagnosis of neurologic complications after HCT.
TA-TMA–directed therapy should be considered in patients with low- or moderate-risk TA-TMA who develop neurologic symptoms.

Abstract
Transplant-associated thrombotic microangiopathy (TA-TMA) and atypical hemolytic uremic syndrome (aHUS) are complement-mediated TMAs. The central nervous system (CNS) is the most common extrarenal organ affected by aHUS, and, despite mechanistic overlap between aHUS and TA-TMA, CNS involvement is rarely reported in TA-TMA, suggesting that CNS involvement in TA-TMA may be underdiagnosed and that these patients may benefit from complement blockers. In addition, there are no widely used histologic or radiologic criteria for the diagnosis of TMA in the brain. Thirteen recipients of pediatric hematopoietic cell transplants (HCTs) who had TA-TMA and who underwent autopsy were studied. Seven of 13 brains had vascular injury, and 2 had severe vascular injury. Neurologic symptoms correlated with severe vascular injury. Classic TMA histology was present and most often observed in the cerebellum, brainstem, and cerebral white matter. Abnormalities in similar anatomic regions were seen on imaging. Brain imaging findings related to TMA included hemorrhages, siderosis, and posterior reversible encephalopathy syndrome. We then studied 100 consecutive HCT recipients to identify differences in neurologic complications between patients with and those without TA-TMA. Patients with TA-TMA were significantly more likely to have a clinical concern for seizure, have an electroencephalogram performed, and develop altered mental status. In summary, our study confirms that TA-TMA involves the brains of recipients of HCT and is associated with an increased incidence of neurologic symptoms. Based on these findings, we propose that patients with low- or moderate-risk TA-TMA who develop neurologic complications should be considered for TA-TMA–directed therapy.
Introduction
Transplant-associated thrombotic microangiopathy (TA-TMA) and atypical hemolytic uremic syndrome (aHUS) are acquired, complement-mediated TMAs. There is significant clinical overlap between these entities, although TA-TMA is more commonly associated with multiorgan injury and death.1 The central nervous system (CNS) is the most common extrarenal organ affected by aHUS, and between 10% and 48% of patients with aHUS have CNS involvement.2-9 Despite the biological similarities between these diseases, neurologic complications in pediatric hematopoietic cell transplant (HCT) recipients are rarely diagnosed as TA-TMA.
A prior study of 202 pediatric HCT recipients reported that 13.5% (n = 27) of patients had neurologic complications in the first 6 months of transplant.10 Neurologic symptoms were most commonly attributed to the effects if calcineurin inhibitors (59%; n = 16), whereas just 2 patients had TA-TMA–related neurotoxicity.10 This large discordance between CNS involvement in TA-TMA and aHUS is unlikely, given the ability of TA-TMA to injure multiple organ systems including the kidneys, bowel, lungs, and even the testicles.1,11,12 A separate study of 221 children and adults noted that patients with TA-TMA were more likely to have neurologic symptoms after HCT than were patients without TA-TMA (40% vs 24%; P = .02).13 These data suggest CNS injury from TA-TMA is underdiagnosed and potentially undertreated. Complement-blocking therapies are an effective TA-TMA treatment and have been used to treat neurologic involvement in various TMAs.14-19 Improved awareness of neurotoxicity from TA-TMA could therefore lead to earlier diagnosis and better outcomes.
Although CNS involvement in aHUS is common, there are currently no established histopathologic or radiologic criteria for the diagnosis of TMA in the CNS. While brain biopsies are rarely performed, detailed knowledge of TMA-mediated vascular injury patterns and the most common locations of these insults would improve our understanding of clinical manifestations of CNS TMA. Similarly, this anatomical knowledge would aid in the interpretation of radiologic studies in patients with suspected CNS TMA.
We hypothesized that brain injury from TA-TMA is clinically underdiagnosed but is histologically and radiographically present in the brains of patients with TA-TMA. To test this hypothesis, we studied autopsy specimens from HCT recipients with TA-TMA and compared histologic and radiographic findings in these subjects. We then studied 100 consecutive HCT recipients to identify differences in neurologic complications between patients with and without TA-TMA.
Methods
Patient selection
We identified patients with TA-TMA who underwent allogeneic or autologous HCT at our institution and had an autopsy performed. All patients were consented to our HCT tissue repository and/or were enrolled in a TA-TMA study that permitted the use of blood and tissue specimens for research. Patients diagnosed with TA-TMA met criteria developed by Jodele et al for TA-TMA and were risk stratified using the same criteria.1,11,15,20 Patients were excluded if no brain tissue was available for review or if available tissue was of insufficient quality for analysis. Chart reviews were performed on these patients and neurologic symptom scores were assigned based on the number of neurologic symptoms present after TA-TMA diagnosis. Neurologic symptoms were selected based on symptoms reported in aHUS neurotoxicity.2 These included seizure, motor neuropathy, sensory neuropathy, ataxia, altered mental status (AMS), vision impairment, and generalized weakness. Each neurologic symptom earned a score of 1 point (eg, 2 symptoms received a score of 2, and 3 symptoms received a score of 3, and so forth).
We also identified 100 consecutive patients who underwent allogeneic or autologous HCT at our institution between 2019 and 2020 to attempt to address the question of whether symptoms of CNS TA-TMA were more frequent than typically appreciated. Chart reviews were performed on these patients for the study of neurologic complications in patients with or without TA-TMA. Neurologic symptoms were chosen based on aHUS literature, as described. Patients with TA-TMA were considered to have neurologic symptoms if those symptoms occurred within 2 weeks before TA-TMA diagnosis and up to 1 year after diagnosis. TA-TMA risk assignment was based on criteria developed by Jodele et al.1,11,15,20 All patients at our institution are prospectively screened for TA-TMA with complete blood counts, lactate dehydrogenase levels, urine protein-to-creatine ratios, and terminal complement levels based on published guidelines.1,11,15,20 Similarly, all patients are treated for hypertension according to our institutional algorithm for HCT recipients which includes personalized blood pressure thresholds based on patient size and age. This work was part of an institutional review board–approved study (ID, 2012-1156) at Cincinnati Children's Hospital Medical Center. The study was conducted in accordance with the Declaration of Helsinki.
Histopathologic tissue and CNS imaging evaluations
All tissue samples were reviewed by a senior pathologist at our institution (S.S.) and graded according to generalized tissue injury and vascular-specific tissue injury. The reviewing pathologist was blinded to all clinical data during her analysis, including TA-TMA risk, terminal complement activation levels, and TA-TMA organ involvement. Overall tissue injury was scored on a scale of 0 to 3, with 0 being absent or insignificant and 3 being severe. Vascular injury was scored on the same scale. Previously published pathology studies of TMA-mediated vascular injury in the kidneys, lungs, and bowel were used to guide our study and scoring.11,21-36 No immunohistochemical stains were used in the scoring process. Brain tissue from a child with no history of TA-TMA or HCT was used as a negative control.
Chart reviews were performed to identify radiologic studies obtained on patients who underwent autopsy and were included in the study. Imaging studies were divided into those performed before or after TA-TMA diagnosis. All radiology studies were reviewed by a senior radiologist (M.M.C.) at our institution and evaluated for abnormalities consistent with TMA-mediated brain injury. Additional clinical complications (eg, infection or tumor metastasis) that could have caused brain imaging abnormalities were considered in this analysis, and we excluded any abnormal brain imaging finding that was clearly attributable to a transplant complication other than TA-TMA. Prior publications on radiographic findings in patients with TMA were used to guide these analyses.2,3,37-43
Statistical analysis
Data are expressed as absolute numbers and percentages, or medians with range or interquartile range. Clinical complications in patients with or without TA-TMA were compared by using Fisher’s exact test. All statistical calculations were performed with GraphPad Prism Software, version 9.
Results
Histopathologic evaluation of brain tissue in patients with TA-TMA
Twenty patients with TA-TMA underwent autopsies and were considered for this study. Thirteen of those patients had adequate brain tissue available to review. Demographics and tissue injury scores for the patients are shown in Table 1. Ten patients were male and 3 were female. The median age at transplant was 14 years old (range, 0.6-29 years). TA-TMA was diagnosed at a median of 19 days after HCT (range, 2-221 days). Six patients were treated with eculizumab, and maximum terminal complement (sC5b-9) measurements ranged from 299 to >1990 ng/mL (normal, <244 ng/mL). Death occurred at a median of 166 days (range, 27-828 days) after HCT, and the most common cause of death was graft versus host disease (GVHD; n = 7). Brain tissue was evaluated for overall tissue injury and vascular-specific injury, then scored from 0 to 3 according to severity (3 being the most severe injury).
Demographics and brain tissue findings at autopsy in pediatric HCT recipients with TA-TMA
| Patient | Diagnosis | Age at HCT (y) | Sex | Transplant type | TA-TMA diagnosis day | TA-TMA risk | Eculizumab therapy | Max sC5b-9 (ng/mL) | Grade 2-4 GVHD | Day of death | Cause of death | Active TA-TMA at death | Maximum urine protein/creatinine ratio in month before death (mg/mg) | Maximum LDH in month before death (relative to upper limit of normal (ULN)) | General tissue injury | Vascular injury | Neurologic symptom score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | XLP | 18 | M | Allogeneic | 39 | Moderate | No | 628 | Yes | 193 | Necrotizing leukoencephalopathy | Yes | 10.5 | 1.5× ULN | 3 | 3 | 4 |
| 2 | HLH | 18 | F | Allogeneic | 3 | Moderate | No | 780 | No | 225 | Bacteremia, sepsis | Yes | 11.5 | 2.3× ULN | 3 | 3 | 3 |
| 3 | NBL | 4 | F | Autologous | 10 | High | No | 880 | No | 27 | Multiorgan failure | Yes | 61.5 | 7.6× ULN | 2 | 2 | 1 |
| 4 | HLH | 0.6 | M | Allogeneic | 160 | High | Yes | 299 | Yes | 247 | GVHD | Yes | 10 | 6× ULN | 2 | 2 | 0 |
| 5 | XLP | 1 | M | Allogeneic | 25 | High | No | 458 | No | 71 | Pneumonitis and ARDS | Yes | 3.5 | 4.5× ULN | 2 | 2 | 0 |
| 6 | XIAP deficiency | 14 | M | Allogeneic | 221 | High | Yes | 385 | Yes | 483 | GVHD | Yes | N/A | 1.9× ULN | 1 | 0 | 3 |
| 7 | WAS | 29 | M | Allogeneic | 20 | High | Yes | 769 | Yes | 164 | GVHD | Yes | 139 | 3.5× ULN | 1 | 0 | 4 |
| 8 | NBL | 3 | M | Autologous | 2 | High | Yes | 420 | No | 61 | Pulmonary fibrosis | Yes | 7.6 | 1.6× ULN | 1 | 1 | 0 |
| 9 | XMEN | 17 | M | Allogeneic | 10 | Moderate | No | >1990 | No | 92 | Multiorgan failure, CMV/EBV | Yes | N/A | 4.1× ULN | 1 | 1 | 2 |
| 10 | AML | 23 | M | Allogeneic | * | * | No | 302 | Yes | 828 | GVHD | Yes | N/A | N/A | 0 | 0 | 0 |
| 11 | Hyper IgE Syndrome | 10 | M | Allogeneic | 154 | High | Yes | 375 | Yes | 166 | GVHD | Yes | 7.4 | 4× ULN | 0 | 0 | 0 |
| 12 | GATA2 mutation | 18 | F | Allogeneic | 18 | Moderate | No | 577 | Yes | 384 | GVHD | Yes | 58.9 | 2.1× ULN | 0 | 0 | 2 |
| 13 | WAS | 0.6 | M | Allogeneic | 11 | High | Yes | 673 | Yes | 110 | GVHD | Yes | 41.1 | 2.8× ULN | 0 | 0 | 0 |
| Patient | Diagnosis | Age at HCT (y) | Sex | Transplant type | TA-TMA diagnosis day | TA-TMA risk | Eculizumab therapy | Max sC5b-9 (ng/mL) | Grade 2-4 GVHD | Day of death | Cause of death | Active TA-TMA at death | Maximum urine protein/creatinine ratio in month before death (mg/mg) | Maximum LDH in month before death (relative to upper limit of normal (ULN)) | General tissue injury | Vascular injury | Neurologic symptom score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | XLP | 18 | M | Allogeneic | 39 | Moderate | No | 628 | Yes | 193 | Necrotizing leukoencephalopathy | Yes | 10.5 | 1.5× ULN | 3 | 3 | 4 |
| 2 | HLH | 18 | F | Allogeneic | 3 | Moderate | No | 780 | No | 225 | Bacteremia, sepsis | Yes | 11.5 | 2.3× ULN | 3 | 3 | 3 |
| 3 | NBL | 4 | F | Autologous | 10 | High | No | 880 | No | 27 | Multiorgan failure | Yes | 61.5 | 7.6× ULN | 2 | 2 | 1 |
| 4 | HLH | 0.6 | M | Allogeneic | 160 | High | Yes | 299 | Yes | 247 | GVHD | Yes | 10 | 6× ULN | 2 | 2 | 0 |
| 5 | XLP | 1 | M | Allogeneic | 25 | High | No | 458 | No | 71 | Pneumonitis and ARDS | Yes | 3.5 | 4.5× ULN | 2 | 2 | 0 |
| 6 | XIAP deficiency | 14 | M | Allogeneic | 221 | High | Yes | 385 | Yes | 483 | GVHD | Yes | N/A | 1.9× ULN | 1 | 0 | 3 |
| 7 | WAS | 29 | M | Allogeneic | 20 | High | Yes | 769 | Yes | 164 | GVHD | Yes | 139 | 3.5× ULN | 1 | 0 | 4 |
| 8 | NBL | 3 | M | Autologous | 2 | High | Yes | 420 | No | 61 | Pulmonary fibrosis | Yes | 7.6 | 1.6× ULN | 1 | 1 | 0 |
| 9 | XMEN | 17 | M | Allogeneic | 10 | Moderate | No | >1990 | No | 92 | Multiorgan failure, CMV/EBV | Yes | N/A | 4.1× ULN | 1 | 1 | 2 |
| 10 | AML | 23 | M | Allogeneic | * | * | No | 302 | Yes | 828 | GVHD | Yes | N/A | N/A | 0 | 0 | 0 |
| 11 | Hyper IgE Syndrome | 10 | M | Allogeneic | 154 | High | Yes | 375 | Yes | 166 | GVHD | Yes | 7.4 | 4× ULN | 0 | 0 | 0 |
| 12 | GATA2 mutation | 18 | F | Allogeneic | 18 | Moderate | No | 577 | Yes | 384 | GVHD | Yes | 58.9 | 2.1× ULN | 0 | 0 | 2 |
| 13 | WAS | 0.6 | M | Allogeneic | 11 | High | Yes | 673 | Yes | 110 | GVHD | Yes | 41.1 | 2.8× ULN | 0 | 0 | 0 |
TA-TMA was diagnosed according to Jodele criteria.1 Histologic grading in each category was performed by a pathologist at our institution. The histologic grading scale is as follows: 0, no or insignificant abnormal findings; 1, mildly abnormal; 2, moderately abnormal; and 3, severely abnormal. Descriptive details on “general” and “vascular” histologic findings are listed in Table 2. Neurologic symptom scores were also generated for these patients. These scores represent the total number of neurologic symptoms present from the following list of symptoms: seizure, AMS, vision change, motor deficit, sensory deficit, and generalized weakness. Active TA-TMA at was defined as laboratory evidence of TA-TMA at the time of death and/or autopsy findings of active TA-TMA.
Patient 10 was diagnosed with TA-TMA at autopsy, not based on laboratory criteria. Patients 6, 9, and 10 did not have a urine protein/creatinine checked within 1 month of death; however, at 2 months before death the ratios were 5.1, 28.4, and 1.8 mg/mg. Because LDH reference ranges vary with age, the LDH maximum is displayed relative to the upper limit of normal for each patient. Patient 10 did not have an LDH checked within 1 month of death; however, at 2 months before death, his LDH was 3× the upper limit of normal. AML, acute myeloid leukemia; ARDS, acute respiratory distress syndrome; CMV, cytomegalovirus; EBV, Epstein-Barr virus; F, female; HLH, hemophagocytic lymphohistiocytosis; LDH, lactate dehydrogenase; M, Male; N/A not available; NBL, neuroblastoma; WAS, Wiskott-Aldrich syndrome; XLP, X-linked lymphoproliferative syndrome; XMEN, X-linked immune deficiency with magnesium defect, Epstein-Barr virus infection, and neoplasia.
Nine of 13 brains had tissue injury (score, ≥1) and 7 brains had vascular injury (score, ≥1). Two patients had a vascular injury score of 3 (severe). Both of them had at least 3 clinical neurologic symptoms and were the only patients to have an overall tissue injury score of 3. Peak sC5b-9 levels in these patients were 628 and 780 ng/mL (normal, <244 ng/mL). Three patients had vascular injury scores of 2 (moderate), although neurologic symptoms in those patients were less common (range, 0-1). The patient with the highest recorded sC5b-9 level (>1990 ng/mL) had a brain vascular injury score of 1 and a neurologic symptom score of 2.
The most common general and vascular histologic findings are shown in Table 2. General observations included global white matter loss, demyelination, and gliosis. Vascular injury findings attributable to TA-TMA included increased vascular wall-to-lumen ratios, vascular wall reduplication, and basement membrane splitting, among others. Representative micrographs of TA-TMA–specific histologic findings are shown in Figure 1A-F and compared with a control brain without TA-TMA (Figure 1G-J). Although we identified classic TA-TMA–mediated vascular injury in 7 of 13 brains, we did not observe any brain-specific histologic manifestations of TA-TMA that would be considered unique from other organ systems affected by TA-TMA. Furthermore, we did not observe any evidence of CNS GVHD, and notably, only 2 of 7 patients with TA-TMA–mediated vascular injury in the brain were diagnosed with GVHD.
A summary of brain histology findings in patients with TA-TMA
| General CNS histology | Vascular histology attributable to TA-TMA | Location of TA-TMA–related changes |
|---|---|---|
|
|
|
| General CNS histology | Vascular histology attributable to TA-TMA | Location of TA-TMA–related changes |
|---|---|---|
|
|
|
General and vascular-specific histologic findings are shown for patients with TA-TMA who underwent autopsy at our institution and had sufficient brain tissue available for examination (n =13). These findings coincide with the general and vascular injury scores shown for each patient in Table 1.
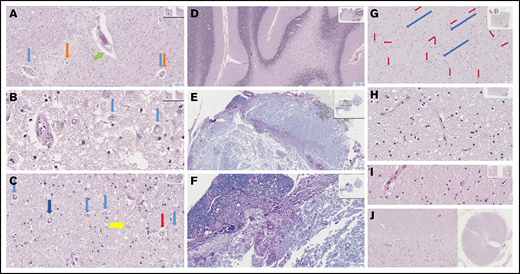
Severe histologic sequelae in the CNS of patients with TA-TMA. Cerebral (A-B; original magnification ×8 (A), original magnification ×40 (B)) and cerebellar (C-D; original magnification x20.5 (C), original magnification ×2.5 (D)) white matter show extensive demyelination, with scattered macrophages (C, yellow arrow, original magnification ×20.5), though not to confluence and not an infarct microscopically or in vascular distribution. Many vessels are affected by chronic changes in other organs that are related to TA-TMA. (C) Capillaries with thickened rigid walls shown at low power, appearing “wire-like” with a ratio of wall to lumen to wall occasionally 1:1:1 (red arrow) are present. (A-C) Capillary basement membrane layering and splitting and pericapillary clearing are also seen (light blue arrows and most pronounced, dark blue arrow). A range of capillaries and small arteries show similar features. Pigment is seen in small capillaries (A, orange arrows) and macrophages are present in the periarteriolar stroma (A, green arrow). (E-F; original magnification ×1.8 (E), original magnification ×8.5 (F)) Loss of myelination is readily evident on Luxol fast blue stain with periodic acid–Schiff highlighting vascular features. (G-J) These findings were compared with the histology in a patient without TA-TMA. There were normal delicate capillaries (red arrows) and tracks (blue arrows), as well as preserved parenchyma in cerebellar (G-H; original magnification x13 (G), original magnification ×40 (H)) and cerebral white (I, original magnification ×40) matter and spinal cord (J, interface of white and gray matter, original magnification ×14/×0.4).
Severe histologic sequelae in the CNS of patients with TA-TMA. Cerebral (A-B; original magnification ×8 (A), original magnification ×40 (B)) and cerebellar (C-D; original magnification x20.5 (C), original magnification ×2.5 (D)) white matter show extensive demyelination, with scattered macrophages (C, yellow arrow, original magnification ×20.5), though not to confluence and not an infarct microscopically or in vascular distribution. Many vessels are affected by chronic changes in other organs that are related to TA-TMA. (C) Capillaries with thickened rigid walls shown at low power, appearing “wire-like” with a ratio of wall to lumen to wall occasionally 1:1:1 (red arrow) are present. (A-C) Capillary basement membrane layering and splitting and pericapillary clearing are also seen (light blue arrows and most pronounced, dark blue arrow). A range of capillaries and small arteries show similar features. Pigment is seen in small capillaries (A, orange arrows) and macrophages are present in the periarteriolar stroma (A, green arrow). (E-F; original magnification ×1.8 (E), original magnification ×8.5 (F)) Loss of myelination is readily evident on Luxol fast blue stain with periodic acid–Schiff highlighting vascular features. (G-J) These findings were compared with the histology in a patient without TA-TMA. There were normal delicate capillaries (red arrows) and tracks (blue arrows), as well as preserved parenchyma in cerebellar (G-H; original magnification x13 (G), original magnification ×40 (H)) and cerebral white (I, original magnification ×40) matter and spinal cord (J, interface of white and gray matter, original magnification ×14/×0.4).
Brain imaging findings in patients with TA-TMA
Chart reviews were performed to identify radiologic studies performed on the 13 patients with TA-TMA whose brain tissue was studied. Eight patients had CNS imaging performed after TA-TMA was diagnosed, and 7 of the patients had CNS imaging before and after TA-TMA diagnosis. Brain abnormalities on imaging studies were common but not universal after TA-TMA diagnosis. Commonly observed brain imaging abnormalities in patients with TA-TMA are shown in Table 3, along with the most common anatomical locations involved. General brain findings on imaging in patients with TA-TMA included parenchymal volume loss and abnormal signal in multiple anatomical locations. Findings attributable to TA-TMA included hemorrhages of various sizes, siderosis, and posterior reversible encephalopathy syndrome (PRES)–related changes.
A summary of brain imaging findings in patients with TA-TMA
| General brain findings | Brain imaging findings attributable to TA-TMA | Location of TA-TMA–related changes |
|---|---|---|
|
|
|
| General brain findings | Brain imaging findings attributable to TA-TMA | Location of TA-TMA–related changes |
|---|---|---|
|
|
|
Brain imaging findings are shown for patients with TA-TMA who underwent autopsy at our institution and had brain imaging obtained before and after TA-TMA diagnosis (n = 7) for comparison. These findings were categorized as “general” or “attributable to TA-TMA.” Parenchymal hemorrhages (gross or micro) in the cortex, deep gray matter, and/or corpus callosum were present in 6 patients. Regional diffusion restriction (n = 5) and PRES (n = 4) were also common findings. One patient had superficial siderosis and multifocal punctate parenchymal hemorrhages.
Representative brain imaging findings from patients with TA-TMA are shown in Figure 2. Patient 1 had a brain vascular injury score of 3 and had prominent abnormalities on brain imaging that were attributable to a vascular process (Figure 2A-G). Magnetic resonance images obtained in the setting of neurologic decline demonstrated new areas of abnormal white matter signal in the periventricular and subcortical white matter. Over a course of 3 months, progressive imaging findings included new cortical signal abnormality with diffusion restriction in the occipital lobes, initially raising concerns for PRES, as well as progressive multifocal brainstem, cerebellar, basal ganglia, and white matter signal abnormalities. Progressive diffusion restriction in the occipital lobes and new, small, intraparenchymal hemorrhages occurred. Patient 3 experienced AMS after autologous HCT for neuroblastoma. Head computed tomography was performed and showed multiple areas of acute hemorrhage (Figure 2H–I). The patient was diagnosed with TA-TMA on the same day, according to laboratory criteria.
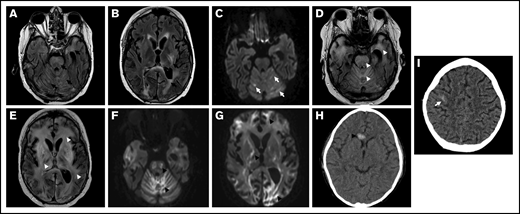
CNS radiographic abnormalities in TA-TMA. An 18-year-old man (patient 1 in Table 1) experienced progressive neurologic decline after HCT and underwent magnetic resonance imaging (A-G) on day 124 after HCT. He was diagnosed with TA-TMA on day 39. (A-B) Axial fluid-attenuated inversion recovery (FLAIR) images demonstrate multifocal areas of signal abnormality (black arrows) in the cerebellum, brainstem, periventricular white matter, and posterior limb of the left internal capsule and adjacent basal ganglia. (C) A T2-trace diffusion–weighted image demonstrates corresponding diffusion restriction predominantly within areas of signal in the cerebellum (white arrows). (D-E) Progressive hyperintense signal abnormality on FLAIR throughout the cerebellum, brainstem, cerebral white matter, and deep gray nuclei (white arrowheads). (F-G) Diffusion-weighted imaging demonstrates corresponding progressive diffusion restriction (black arrowheads). A 4-year-old patient with neuroblastoma (patient 3 in Table 1) experienced altered mental status on day 10 after autologous HCT and underwent a head CT (H-I). TA-TMA was diagnosed on the same day. Axial computed tomographic images demonstrate a new, ovoid, high-attenuation hemorrhage in the genu of the corpus callosum (arrowhead), as well as a more subtle hemorrhage along the cortical surface of the posterior right frontal lobe (arrow).
CNS radiographic abnormalities in TA-TMA. An 18-year-old man (patient 1 in Table 1) experienced progressive neurologic decline after HCT and underwent magnetic resonance imaging (A-G) on day 124 after HCT. He was diagnosed with TA-TMA on day 39. (A-B) Axial fluid-attenuated inversion recovery (FLAIR) images demonstrate multifocal areas of signal abnormality (black arrows) in the cerebellum, brainstem, periventricular white matter, and posterior limb of the left internal capsule and adjacent basal ganglia. (C) A T2-trace diffusion–weighted image demonstrates corresponding diffusion restriction predominantly within areas of signal in the cerebellum (white arrows). (D-E) Progressive hyperintense signal abnormality on FLAIR throughout the cerebellum, brainstem, cerebral white matter, and deep gray nuclei (white arrowheads). (F-G) Diffusion-weighted imaging demonstrates corresponding progressive diffusion restriction (black arrowheads). A 4-year-old patient with neuroblastoma (patient 3 in Table 1) experienced altered mental status on day 10 after autologous HCT and underwent a head CT (H-I). TA-TMA was diagnosed on the same day. Axial computed tomographic images demonstrate a new, ovoid, high-attenuation hemorrhage in the genu of the corpus callosum (arrowhead), as well as a more subtle hemorrhage along the cortical surface of the posterior right frontal lobe (arrow).
Six patients demonstrated parenchymal hemorrhages in the cortex, deep gray matter, and/or corpus callosum. Regional areas of diffusion restriction were present in 5 patients. One patient had superficial siderosis and multifocal punctate parenchymal hemorrhages. Four patients presented with imaging findings concerning for PRES within weeks of their TMA diagnosis.
Neurologic symptoms in patients with TA-TMA
We studied 100 consecutive patients who underwent HCT at our institution from 2019 through 2020, to determine the prevalence of symptoms in a nonselect population representative of our clinical practice. Allogeneic and autologous HCTs were both included in this cohort. Twenty-eight patients were diagnosed with moderate- or high-risk TA-TMA, 17 of whom had high-risk TMA, according to the Jodele criteria.20 Thirteen patients received eculizumab for therapeutic inhibition of terminal complement. Mortality was significantly higher (P = .0004) in patients with TA-TMA (29.03%; n = 9 deaths) compared with patients without TA-TMA (4.35%; n = 3 deaths). Follow-up time after HCT ranged from 1 to 2 years. Patients with TA-TMA were also significantly more likely to require transfer to the intensive care unit (P = .008) and intubation (P = .0004). Neurologic complications for these patients are shown in Table 4.
Neurologic complications and outcomes in pediatric TA-TMA
| Moderate or high-risk TA-TMA, % (n) (n = 28) | No TA-TMA % (n) (n = 72) | P | |
|---|---|---|---|
| Neurology consult requested | 28.5 (8) | 15.3 (11) | 0.15 |
| Clinician concern for seizure | 25 (7) | 5.6 (4) | 0.01 |
| EEG performed | 21.4 (6) | 2.8 (2) | 0.006 |
| Seizure captured on EEG | 7.1 (2) | 1.4 (1) | 0.19 |
| Stroke | 0 (0) | 1.4 (1) | >0.99 |
| PRES | 10.7 (3) | 1.4 (1) | 0.07 |
| AMS | 50 (14) | 18.1 (13) | 0.002 |
| Ophthalmology consult requested | 46.4 (13) | 33.3 (24) | 0.25 |
| ICU admission/transfer | 67.9 (19) | 37.5 (27) | 0.008 |
| Intubated | 42.9, (12) | 9.7 (7) | 0.0004 |
| Expired | 32.1 (9) | 4.2 (3) | 0.0004 |
| Moderate or high-risk TA-TMA, % (n) (n = 28) | No TA-TMA % (n) (n = 72) | P | |
|---|---|---|---|
| Neurology consult requested | 28.5 (8) | 15.3 (11) | 0.15 |
| Clinician concern for seizure | 25 (7) | 5.6 (4) | 0.01 |
| EEG performed | 21.4 (6) | 2.8 (2) | 0.006 |
| Seizure captured on EEG | 7.1 (2) | 1.4 (1) | 0.19 |
| Stroke | 0 (0) | 1.4 (1) | >0.99 |
| PRES | 10.7 (3) | 1.4 (1) | 0.07 |
| AMS | 50 (14) | 18.1 (13) | 0.002 |
| Ophthalmology consult requested | 46.4 (13) | 33.3 (24) | 0.25 |
| ICU admission/transfer | 67.9 (19) | 37.5 (27) | 0.008 |
| Intubated | 42.9, (12) | 9.7 (7) | 0.0004 |
| Expired | 32.1 (9) | 4.2 (3) | 0.0004 |
Patients with moderate- or high-risk TA-TMA were compared with patients without TA-TMA, according to criteria developed by Jodele et al.1,11,15,20 All complications occurred after stem cell infusion. Complications in the moderate- or high-risk TA-TMA group occurred either after TA-TMA diagnosis (but within 1 year of diagnosis) or within 2 weeks before TA-TMA diagnosis. Complications that occurred more than 2 weeks before TA-TMA diagnosis were excluded from the moderate or high-risk TA-TMA group. Clinical concern for seizure was determined based on clinician documentation in patient charts. P values were generated by Fisher’s exact test. EEG, electroencephalogram, ICU, intensive care unit. 2. Bold values indicate values that were statistically significant with a P value cutoff of < 0.05.
The most common neurologic symptom was AMS and was seen in 27% of all HCT recipients. Patients with TA-TMA were significantly more likely to have AMS (P = .002), a clinical concern for seizure (P = .01), and an electroencephalogram performed (P = .006). The median maximum sC5b-9 level in patients with TA-TMA was 408.5 ng/mL (interquartile range, 289.5-682.8 ng/mL; normal range, <244 ng/mL) and 32% (8 of 25) of allogeneic HCT recipients with TA-TMA had grade 3 to 4 GVHD. Neurology was consulted in 19% of all HCT recipients. Twenty-eight percent of patients with TA-TMA required a neurology consult compared with 15% of patients without TA-TMA; however, this result was not statistically significant (P = .15). PRES was more common in patients with TA-TMA than in patients without TA-TMA, but was not statistically significant in this sample size (10.7% vs 1.4%; P = .07). Only 1 patient in this cohort was diagnosed with a stroke, and that patient did not have TA-TMA. There was no difference in generalized weakness, motor neuropathy, sensory neuropathy, or ataxia between these groups. Ophthalmology consults were requested in 46.4% of patients with TA-TMA compared with 33.3% of patients without TA-TMA; however, the difference was not statistically significant (P = .25), and further review of the indications for consult did not identify a trend related to TA-TMA.
Neurologic symptom assessment algorithm in TA-TMA
The observed radiologic, histologic, and neurologic symptom findings suggest CNS TA-TMA is underdiagnosed. We therefore propose a TA-TMA management algorithm that incorporates the presence of neurologic symptoms and/or brain-imaging abnormalities into the decision process for TA-TMA–directed therapy (Figure 3). This algorithm recommends that TA-TMA–directed therapy be considered in patients with low- or moderate-risk TA-TMA who have neurologic complications and otherwise would not receive TA-TMA–directed therapy according to current data.1,11,15
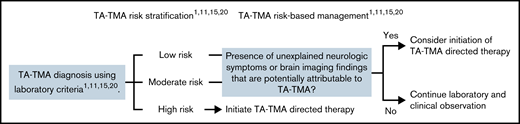
A modified TA-TMA management algorithm that incorporates CNS manifestations of TA-TMA in treatment decisions. As previously published, low risk TA-TMA is limited to laboratory evidence of intravascular hemolysis without end organ injury or increased terminal complement activation.1,11,15,20 Moderate risk TA-TMA is defined as the presence of either a random urine protein creatinine ratio >2 mg/mg or an elevated plasma sC5b-9 level (terminal complement, normal range <244 ng/mL).1,11,15,20,53 High-risk TA-TMA includes patients with both of these laboratory abnormalities as well as patients with TA-TMA diagnosed on tissue biopsy.1,11,15,20 We propose the inclusion of neurologic symptoms or brain imaging findings potentially attributable to TA-TMA into the treatment decision process, as these patients may have CNS TA-TMA and early initiation of complement inhibitors may limit morbidity from TA-TMA–mediated brain injury.
A modified TA-TMA management algorithm that incorporates CNS manifestations of TA-TMA in treatment decisions. As previously published, low risk TA-TMA is limited to laboratory evidence of intravascular hemolysis without end organ injury or increased terminal complement activation.1,11,15,20 Moderate risk TA-TMA is defined as the presence of either a random urine protein creatinine ratio >2 mg/mg or an elevated plasma sC5b-9 level (terminal complement, normal range <244 ng/mL).1,11,15,20,53 High-risk TA-TMA includes patients with both of these laboratory abnormalities as well as patients with TA-TMA diagnosed on tissue biopsy.1,11,15,20 We propose the inclusion of neurologic symptoms or brain imaging findings potentially attributable to TA-TMA into the treatment decision process, as these patients may have CNS TA-TMA and early initiation of complement inhibitors may limit morbidity from TA-TMA–mediated brain injury.
Discussion
Neurologic complications are a major cause of morbidity and mortality in aHUS2 ; however, the incidence and clinical manifestations of neurotoxicity from TA-TMA are unclear. We evaluated histologic and radiographic abnormalities in patients with TA-TMA and reported differences in neurologic complications in patients with or without TA-TMA. This is the first study, to our knowledge, that specifically evaluated histologic, radiologic, and clinical findings related to CNS TA-TMA.
The results confirm that TA-TMA frequently injures the CNS vasculature and found that 38% of patients with TA-TMA had moderate or severe CNS vascular injury at autopsy. Brain biopsies are rarely obtained, limiting CNS histology studies and the development of evidence-based diagnostic criteria for TMA-mediated brain injury in both transplant-associated and non–transplant-associated TMA. We observed classic vascular injury patterns of TMA in the brains of HCT recipients, which confirmed the presence of CNS TA-TMA in this patient population. A recent study of neurologic complications in patients with COVID-19 included 2 patients who underwent brain biopsy.44 Both patients had overt histologic evidence of TMA described as vascular wall alterations (specifically in small arterioles, capillaries, and venules), disappearance of endothelial cells, and local (but not vascular wall) inflammation.44 These findings further supports the histologic evidence reported in our study and exemplifies the widespread applicability of the findings to nontransplant cases of TMA.
A correlation was seen between HCT recipients with the most severe vascular injury at autopsy and the number of neurologic symptoms present in those patients. However, patients with moderate vascular injury at autopsy had either 1 (n = 1) or no (n = 2) neurologic symptoms. This observation could suggest that CNS injury from TA-TMA is not always permanent or clinically manifested, although definitive conclusions are limited by the small sample size. Related to this observation is the fact that the duration of time between initial TA-TMA diagnosis and autopsy varied markedly across the different patients in our study. This variance could affect the histologic manifestations of TA-TMA in our cohort. It is conceivable that chronic TA-TMA can cause more chronic vascular injury patterns in comparison with a treatment-responsive, short-duration TA-TMA. Because more patients now survive TA-TMA than in prior decades, we must continue to study the potential long-term implications of both acute and chronic vascular changes related to TA-TMA.
Generalized cerebral white matter and cerebellar involvement were common in our specimen reviews and are anatomically consistent with known symptoms of CNS TMA, such as seizure, headache, altered mental status, and ataxia. Brainstem injury on imaging has been reported in patients with aHUS and HUS. However, brainstem injury is rarely attributed to TA-TMA in current clinical practice. Our tissue findings support the presence of TA-TMA–mediated brainstem injury in patients who undergo HCT and are consistent with aHUS and HUS literature that describe the brainstem as a target of CNS TMA.37,39,41-43 TA-TMA should therefore be included in the differential diagnosis of respiratory failure and other brainstem-related complications in patients at risk for developing or already diagnosed with TA-TMA.
Grade 2 to 4 GVHD was common in the autopsied cohort, and it is therefore necessary to consider GVHD to be a potential confounding cause of vascular injury in these patients. Importantly, the described vascular injury patterns were observed in both autologous HCT recipients included in the autopsy study. This validates that these were not GVHD-mediated findings because autologous HCT recipients are not at risk for GVHD. In addition, only 2 of the 7 patients with TA-TMA–mediated vascular injury had a diagnosis of GVHD. CNS findings in patients with GVHD have been reported in a handful of publications and are most commonly described as vasculitis with perivascular lymphocytic infiltration.45-50 We did not observe any lymphocytic vasculitis, nor did we identify any other manifestations of GVHD in the studied brain tissue.
It is also conceivable that specific TA-TMA triggers (eg, viral infections and exposure to drugs or conditioning chemotherapy) are important in the pathogenesis of CNS TA-TMA. Dvorak et al proposed a “3-hit hypothesis” for the development of TA-TMA, which includes a predisposition to complement activation/preexisting endothelial injury (first hit), endothelial injury from conditioning chemotherapy (second hit), and post-HCT endothelial injury from infection, alloreactivity or other causes (third hit).51 Furthermore, Jodele et al published an updated risk stratification for TA-TMA that identifies concurrent grades 2 to 4 GVHD as a high-risk feature of TA-TMA.52 These findings suggest the exact type of hits present are important in the disease progression of TA-TMA. Because of the limited number of patients in the autopsy study, we were unable to investigate these specific hits and their impact on CNS TA-TMA, and we therefore recommend further investigation.
Imaging abnormalities in patients with neurologic complications from aHUS or HUS have been described in the deep white matter, basal ganglia, and brainstem on diffusion-weighted MRI.2 Similar findings were noted on images in our study and correlated with areas of brain injury observed at autopsy in those patients. The diagnostic specificity of these findings in isolation is limited; however, in combination with a risk for TA-TMA or an existing TA-TMA diagnosis, these could be diagnostic of CNS TA-TMA. Although kidney injury is classically associated with aHUS, clinical manifestations of extrarenal organ injury can occur before kidney injury, and extrarenal organs may be more severely affected in some patients.3,53-55 It is therefore feasible that certain patients with TA-TMA will present with isolated neurologic symptoms. Neuroimaging findings in these patients may aid in the decision to start complement-blocking therapies in patients who may otherwise not meet traditional criteria for TA-TMA treatment. This study showed that there is a spectrum of imaging findings in patients with TA-TMA which makes diagnosis on imaging alone difficult. However, brain imaging findings such as PRES, multifocal cortical and white matter hemorrhages, or other nonspecific hemorrhages in conjunction with appropriate clinical and laboratory findings can support the diagnosis of CNS TA-TMA.
In our neurologic symptom study we found that patients with TA-TMA were more likely to develop neurologic complications after TA-TMA diagnosis than were patients without TA-TMA at any point in their transplant course. Although this finding is limited to an association, it suggests that clinically relevant neurologic consequences from TA-TMA exist and are underdiagnosed, even at our center which has a major research focus on TA-TMA. This hypothesis is further supported by our autopsy findings, which clearly showed TA-TMA–mediated brain injury. We did not observe a relationship between the magnitude of sC5b-9 elevation and neurologic symptom development; however, this investigation was limited by the ability to retrospectively associate specific neurologic symptoms with TA-TMA. Terminal complement generation may also be dependent on the physical size of injured tissue, and therefore brain injury from TA-TMA may not generate as much terminal complement as larger organs (eg, bowel).
Improved diagnosis of CNS TA-TMA can be achieved by increased clinical awareness, improved symptom recognition, and the use of CNS imaging as a diagnostic tool. Morbidity and mortality from CNS TA-TMA are largely unknown because of a lack of standardized diagnostic criteria; however, we speculate that early initiation of TA-TMA–directed therapy in these patients is likely to improve outcomes. We therefore propose a modified treatment algorithm for patients with TA-TMA that expands consideration of TA-TMA–directed therapy to moderate- and low-risk patients with TA-TMA with neurologic symptoms or brain imaging abnormalities. Importantly, we acknowledge that the neurologic symptoms described in this study are not specific to TA-TMA, and a concurrent workup for other post-transplant neurologic complications (eg, infection or stroke) is crucial.
The histology portion of this study was limited by the use of autopsy specimens, which can introduce tissue-processing and postmortem artifacts. However, given the rarity of brain biopsies, these specimens were thought to be the only feasible tissue source for our study. Although fresh biopsy tissue is preferred, postmortem and/or processing artifacts were not felt to be relevant to our histologic observations, as cases with advanced postmortem degeneration were excluded. The described vascular findings are specific to TMA-mediated endothelial injury and are not thought to be influenced by tissue source. Furthermore, we commonly observed a deposition of hemosiderin that is consistent with longstanding microhemorrhage rather than acute injury from postmortem processing.1,21 Our brain imaging studies were limited by inconsistent imaging timing and frequency relative to TA-TMA diagnosis and HCT. However, we focused our conclusions on the 7 patients with imaging before and after TA-TMA diagnosis, so that informative comparisons were possible. Last, our neurologic symptom analysis was limited by its retrospective format and the lack of a defined link between neurologic symptoms and TA-TMA, largely because of poor awareness of neurologic symptoms in TA-TMA and the absence of diagnostic criteria for neurologic symptoms in TA-TMA, which this study seeks to improve.
In summary, our study confirmed that TA-TMA involves the brains of HCT recipients and is associated with an increased incidence of neurologic symptoms. Prospective studies are needed to better define the neurologic symptoms most indicative of TA-TMA and to further characterize diagnostic imaging abnormalities in patients with TA-TMA. Biomarkers of CNS TMA (eg, sC5b-9 measurement in cerebrospinal fluid) are also needed; however, these will be limited by the ability to perform lumbar punctures in patients with TA-TMA or suspected TA-TMA. Future studies of brain tissue specimens in patients with complement-mediated TMAs should also evaluate the role of complement staining (eg, C4d, sC5b9) in the diagnosis of brain injury from complement-mediated TMA. Based on the current study findings, we propose that patients who are diagnosed with low- or moderate-risk TA-TMA and develop neurologic complications be considered for TA-TMA–directed therapy.
Acknowledgments
The authors thank the patients and families of patients who were included in this study for their commitment to research and improving outcomes for pediatric hematopoietic cell transplant recipients. This work was supported in part by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under Grant R01 HD093773 (principal investigator, S.J.).
Authorship
Contribution: A.S. wrote the manuscript, designed the study, performed chart reviews, and performed statistical analyses; G.A. performed chart reviews. S.S. reviewed and interpreted all pathology specimens and designed the pathology figures; M.M.C. reviewed and interpreted all imaging studies, edited the manuscript, and designed the radiology figures; C.E.D. offered TMA expertise, performed chart reviews, and reviewed and edited the manuscript; S.M.D. designed the study, wrote the manuscript, and edited the figures; and S.J. oversaw the study, performed chart reviews, and reviewed and edited the manuscript and figures.
Conflict-of-interest disclosure: A.S. has consulted for SOBI. S.J. holds US Patent 10815 296 B2, “Methods of treatment of HSCT-associated thrombotic microangiopathy with eculizumab;” has received research support from Alexion Pharmaceuticals; and has had consultancies with Omeros, SOBI, and Alexion. S.M.D. has received research support from Alexion Pharmaceuticals and has had consultancies with Novartis, Rocket Pharma, CIRM, Allovir, and Neurogene. S.J. is a coinventor on US Patent PCT/US2014/055922 “Compositions and Methods for Treatment of HSCT-Associated Thrombotic Microangiopathy.” The remaining authors declare no competing financial interests.
Correspondence: Anthony Sabulski, Cancer and Blood Diseases Institute, Cincinnati Children’s Hospital Medical Center 3333 Burnet Ave, Cincinnati, OH 45229; e-mail: anthony.sabulski@cchmc.org.

