

Abstract
Radioimmunotherapy (RIT) with 90Y-Zevalin® combined with high dose therapy and autologous stem cell transplantation (ASCT) is gaing increasing importance for the treatment of relapsed or refractory non Hodgkin Lymphoma (nHL). We evaluated the feasibility and the clinical results of the addition of 90Y-Zevalin® at standard dose to BEAM regimen (Z-BEAM) in nHL pts who failed to achieve complete remission (CR) after previous chemoimmunotherapy.
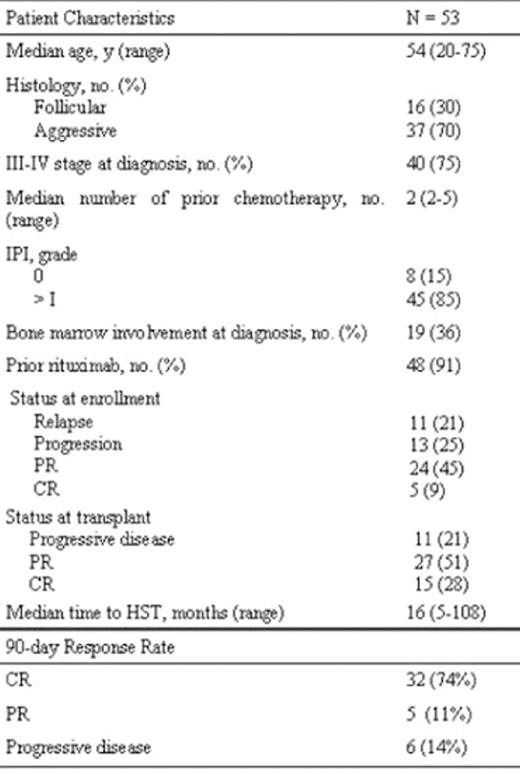
Methods. Between October 2005 and June 2008, 53 patients were enrolled in 11 italian centers. The treatment strategy is shown in figure 1. Salvage treatment consisted of 2 courses of R-DHAP. PBSCs were collected after mobilization with DHAP and G-CSF plus in vivo purging with Rituximab. Patients’ characteristics are shown in table 1.
Results. The median CD34+ cells infused was 5.5 x10^6/Kilograms (range 2.55–34). All patients engrafted. The median number of red blood cell and platelet transfusion were 4 (1–7) and 6 (1–8), respectively. The median time to platelet and neutrophil counts higher than 20x10^9/L and 0.5x10^9/L were 14 (range, 9–60 days) and 10 days (range, 8–20), respectively. Mucosites occurred in all pts (grade III in 20 and grade IV in 5 patients). Febrile neutropenia occurred in 39 pts (74%). Eight pneumonitis and 12 blood stream infections, mainly by Gram+, were documented. One patient developed an atrial fibrillation. Five pts were not evaluable for response because too early. The 90-day overall response rate was 86% with 74% of CR. Three relapses (relapse rate 9%) and four progression were documented at a median follow-up of 247 days post Z-BEAM (range, 125–818). The potential factor to predict CR was: at last PR before Z-BEAM (p=0.06). Fourthy patients are alive at a median follow-up of 175 days post HST (range, 6–590): thirty pts in CR (57%), three pts in PR (5.5%), three pts in progressive disease (PD, 6%)(fig. 2). Fourtheen pts died (26%): 5 deaths due to TRM before day 90, 1 for ARDS (+230), 1 TRM post a subsequent RIC allotransplant (+95) and 6 due to PD (median follow-up 110 days, range 97–150). The Kaplan-Meyer estimated 3y-EFS is 64%. Five early deaths before day-90 occurred: 2 due to septic shock (day +6 and +39), 1 to pneumonitis (+22), 1 for BK viral encephalites (+61) and 1 to MOF (+14). The Kaplan-Meyer estimated Treatment Related Mortality (TRM) is 9.3%. Two statistically risk factors for 90-day TRM (p<0.03) were documented: age elderly then 65 and non follicular lymphomas histology. Cox multivariate regression analysis demonstrated that age more than 65 is a significant risk factor for TRM (3.4% in pts aged less then 65 years and 21,05% in older pts; p<0.01).
Conclusion. In pts with different histology nHL, who failed to achieve CR after previous immuno-chemotherapy, RIT integrated with high-dose chemotherapy (Z-BEAM) is capable to induce 86% of ORR, 74% of CR and 3 ys EFS of 64%, with sustained engraftment and an acceptable extra-haematological toxicity, mainly restricted to pts older then 65 ys. The power of this program needs to be assessed in a larger series of patients and in a randomized fashion.
Table 1: Patient Characteristics and 90-day response post HST

Disclosures: No relevant conflicts of interest to declare.

