

Abstract

Flow cytometry for detection of minimal residual disease (MRD) in acute lymphoblastic leukemia (ALL) has been widely used in pediatric patients to quantify therapeutic response and to assess the risk of relapse. Flow cytometry for MRD provides roughly the same level of sensitivity (0.01%) as molecular methods but at lower cost and with faster turnaround time. MRD assessment in ALL currently requires an evaluation of 20 or more parameters divided among multiple tubes.
In part due to the assessment complexity, the use of flow cytometry for MRD detection in adult ALL patients has been relatively limited. We developed a 6-color, single-tube, flow cytometry assay to detect MRD in bone marrow (BM) aspirate specimens from adult ALL patients. The 73 patients included 52 patients with B-ALL (71%), 19 patients with T-ALL (26%) and 2 patients with T/myeloid leukemia (3%) and were treated with one of several standard chemotherapeutic regimens or targeted therapies. Patients were tested for MRD by flow cytometry after induction or re-induction therapy and serially thereafter. The 6-marker MRD panel was customized for each patient based on the 18-20-marker diagnostic immunophenotype.
Sixty-three percent of B-ALL patients (n=33) had lymphoblasts with an aberrant immunophenotype; expression of a myeloid marker (e.g., CD13, CD15 or CD33) was the most common aberrancy. The remaining 37% of B-ALL patients (n=19) had disease with a hematogone immunophenotype, which comprised surface expression of CD10, CD19, CD20, CD34, CD38 and CD45; in the majority of these cases, leukemic cells were distinguishable from normal hematogones based on the intensity of surface marker expression. Forty-seven percent of T-ALL patients (n=9) had an aberrant immunophenotype, most often characterized by CD33 expression.
One-hundred forty-six consecutive specimens analyzed for MRD by flow cytometry were classified as positive (23%), negative (72%) or uncertain (5%). Of the 34 samples classified as positive, 14 (41%) showed morphologic (i.e., BM aspirate or biopsy) evidence of disease; nineteen (65%) samples did not show morphologic evidence of disease and 1 sample did not have a concurrent morphologic assessment. Of the 105 samples classified as negative by flow cytometry, 103 (98%) were also negative by morphology and 1 sample did not have a concurrent morphologic assessment. One sample that was negative by flow cytometry had morphologic evidence of disease in the biopsy (10-20% blasts) but not the aspirate, suggesting that aspirate sampling artifact was responsible for the discrepancy. None of the 7 samples classified as uncertain by flow cytometry had morphologic evidence of disease; five out of 7 uncertain classifications were in B-ALL patients with hematogone immunophenotypes. Overall, MRD flow cytometry showed 86% concordance with the results of morphologic assessment.
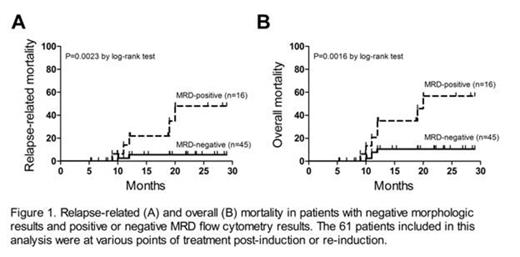
We evaluated outcomes in all patients with negative morphologic results and any positive MRD flow cytometry result(s). Of the 73 patients in this study, 61 had morphology-negative results that were either MRD-negative (n=45) or MRD-positive (n=16). Patients in this group were at various points of treatment post-induction or re-induction. Four out of 45 patients (9%) with MRD-negative results relapsed during a median follow-up period of 22 months, and 8 out of 16 patients (50%) with an MRD-positive result relapsed during a median follow-up period of 15 months (odds ratio for relapse 10.3, 95% confidence interval 2.5-42.4, P=0.001). In addition, relapse-related and overall mortality (Figure 1) were higher in patients with MRD-positive results (P=0.0023 and P=0.0016, respectively, by the log-rank test).
In summary, we present a simplified, single-tube, flow cytometry assay that can be used to detect MRD in adult ALL at relatively low cost with rapid turnaround time; our approach was applicable to cases with either hematogone or aberrant immunophenotype, yielding a definitive result in 95% of cases. Notably, the presence of MRD was associated with relapse and mortality, suggesting that our method of MRD assessment could be used to guide treatment of adult ALL. Further analysis of the correlations between MRD results, clinical management and patient outcomes is ongoing.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

