

Abstract
Introduction
Hemophagocytic lymphohistiocytosis (HLH) is an immune-mediated life-threatening condition in which activated macrophages phagocytize hematopoietic cells in various clinical situations from physiologic reactions to pathologic conditions such as malignancy. The diagnosis of HLH is currently done according to the HLH-2004 criteria which were mainly based on pediatric experiences even though underlying causes and clinical features of adult patients with HLH are different from pediatric patients. However, there is little information about the value of each item and its clinical relevance in the diagnosis of adult patients. Thus, we analyzed the diagnostic value of HLH-2004 criteria in adult patients who had symptoms or signs suspicious of hemophagocytosis.
Methods
We have conducted a prospective cohort study for adult HLH since January of 2017 (Prospective cohort for adult hemophagocytosis: NCT03117010). Adult patients older than 18 years having at least one of the following problems could be enrolled onto this prospective cohort: 1) Pathologically confirmed hemophagocytosis in bone marrow or lymph nodes; 2) Presence of at least 3 conditions among 8 items of HLH-2004 diagnostic criteria. After obtaining written informed consent, we performed laboratory tests for the diagnosis of HLH including natural killer (NK)-cell activity and soluble CD25 in blood. The primary objective of this study was to explore the feasibility and clinical usefulness of HLH-2004 criteria in adult patients, and secondary objective was to analyze underlying causes and outcomes of adult HLH.
Results
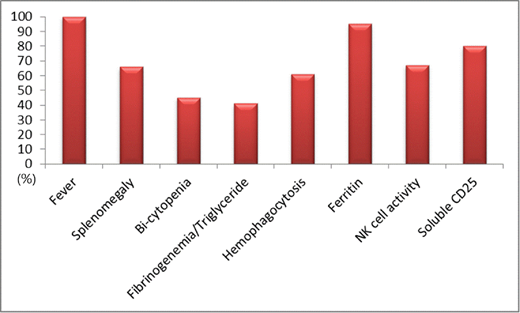
At the time of analysis, 44 patients were enrolled in the cohort, and their median age was 51.5 years (range, 19-85 years). Male (n=27) was more common than female (n=17). All patients had fever (body temperature ≥ 38.5°C) and splenomegaly was found in 29 patients (66%, Figure 1). Although cytopenia such as neutropenia and thrombocytopenia was commonly found, only 20 patients had bi-lineage cytopenia (45%). Hypofibrinogenemia and/or hypertriglyceridemia were also less common findings (n=18, 41%). Hemophagocytosis in bone marrow or lymph nodes was pathologically confirmed in 27 patients (61%). Elevated serum level of ferritin (≥ 500 mg/L) and soluble CD25 (≥ 2400 U/mL) were 42 (95%) and 35 patients (80%), respectively. Among 33 patients whose NK-cell activity was evaluated, 22 patients had low or absent NK-cell activity (67%). According to diagnostic criteria, 28 patients having at least five conditions were diagnosed with HLH, and the remaining patients including 7 patients with bone marrow hemophagocytosis could not be diagnosed. Among 28 patients with HLH, T/NK-cell (n=8) and B-cell lymphomas (n=7) were the most common underlying disorders (n=15, 54%). Infection including EBV (n=6) and rheumatologic disorders (n=3) accounted for non-malignancy associated HLH whereas the remaining four patients' cause was not identified. At the time of analysis, 14 patients died due to uncontrolled HLH or underlying disorders or infectious complications during treatment. The median overall survival of all patients was 13.9 months (95% CI: 10.9 - 16.9), and patients with HLH was not significantly different from patients without HLH (p=0.655). The survival outcome of patients with lymphoma was significantly worse than patients without it regardless of HLH diagnosis (p<0.001).
Conclusions
Fever and elevated level of serum ferritin were the most frequent condition in patients having suspicious symptoms of HLH. Low or absent NK-cell activity and increased level of soluble CD25 could have additional diagnostic value for timely diagnosis of adult HLH. Considering lymphoma is frequently associated with adult HLH, immediate evaluation for lymphoma should be done in adult patients suspicious of HLH.
No relevant conflicts of interest to declare.

