

Abstract

Introduction:
The presence of pulmonary hypertension (PH) in myeloproliferative disorders (MPD) has been evaluated in several small studies with mainly echocardiographic assessment of the right ventricular systolic pressures (RVSP). Left-sided heart disease is the most common cause of PH, and the incidence of diastolic dysfunction increases with age. Since MPD is more prevalent in older patients, it is unknown how much of PH is related to diastolic dysfunction. In addition, the presence and effect of concomitant cardiovascular diseases on overall mortality in these patients is unknown. To assess above knowledge gaps, we evaluated the relationship of PH, cardiovascular diagnoses and echocardiographic findings in a population of patient with myelofibrosis (MF).
Methods:
Data from MF patients who underwent formal echocardiogram from 10/1/2015 to 5/20/2017 at MD Anderson Cancer Center was collected. Clinical, radiographic, laboratory and echocardiographic data were reviewed. We performed Kaplan-Meier survival analysis focusing on cardiovascular diagnoses, laboratory values and echocardiographic variables. We determined a variable to be statistically significant from Kaplan-Meier if p-value from Log Rank (Mantel-Cox) was <0.05. Statistical software used was SPSS.
Results:
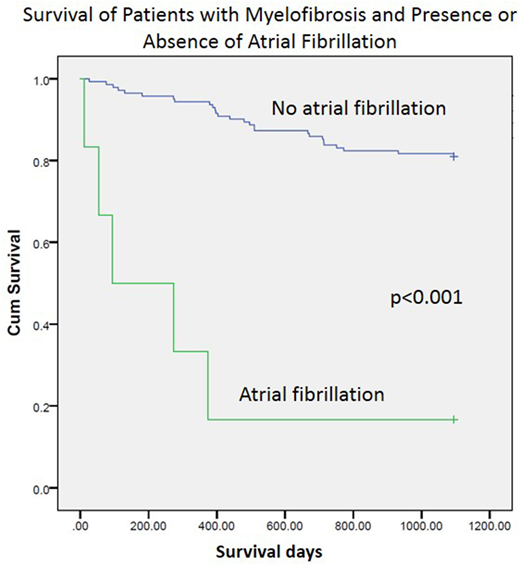
One hundred fifty-one patients (72 females, 79 males) were identified. The median age was 68.5 ± 14.09 years. ECOG performance status was 0 (38%), 1 (55%) and 2 (6%). Splenomegaly was present in 36%, and 40% were undergoing active treatment. Respiratory complaints included dyspnea (13%), lower extremity edema (6%) but no chest pain or syncope. Comorbid conditions included hypertension (57%), hypothyroidism (25%), dyslipidemia (23%), chronic kidney disease (12%), coronary artery disease (11%), diabetes (9%), atrial fibrillation (AF) (4%) and thromboembolic disease (7%). RVSP data was available in 103 patients. Evidence of PH by echocardiogram was found in 20%, and PH with normal diastolic function (presumptively pre-capillary PH) was found in 6%. Laboratory data revealed median hemoglobin 10.4 gm/dL (5.2-116.6), white blood cell count 8.7 x 10 K/uL (1.7-156.9), and platelets 227 K/uL (14-1432). No right heart catheterization was performed. Survival analyses revealed that a diagnosis of AF, a dilated left atrium (>34 mL/m2) and a low RVs' (<10 cm/s) (parameter of RV systolic function) were associated with a worse prognosis, and the strongest association with mortality was AF (p<0.001). The presence of other comorbidities, PH by echocardiogram, increased right ventricle size or decreased left ventricular systolic function were not statistically significant for increased mortality.
Conclusion:
In our cohort of MF, the incidence of pre-capillary PH on echocardiogram was 6%. The presence of AF and echocardiographic findings of left atrial dilatation and decreased RV systolic dysfunction by RVs' are strongly related to worse prognosis. Of which the presence of AF was the most robust. Traditional PH variables in echocardiogram are not related to overall prognosis in this population. Further study is needed to evaluate the impact of cardiovascular disease in MF.
Verstovsek:Celgene: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Italfarmaco: Membership on an entity's Board of Directors or advisory committees; Incyte: Consultancy.
This icon denotes a clinically relevant abstract

