

Abstract
Introduction:
In CLL, chemoimmunotherapies (CIT) and combinations with novel agents have proven to be highly effective with regard to eradication of minimal residual disease (MRD), while complete remissions (CR) are frequently not achieved due to residual lymphadenopathy. We have previously reported that minimal residual disease (MRD) negativity after CIT is a prognostic factor irrespective of the clinical response (Kovacs et al., JCO 2016). Because inferior outcome was observed in small subgroups of patients (pts) with residual lymphadenopathy, we analyzed the prognostic value of residual lymphadenopathy after CIT in comparison to MRD detection in a larger pt population.
Methods:
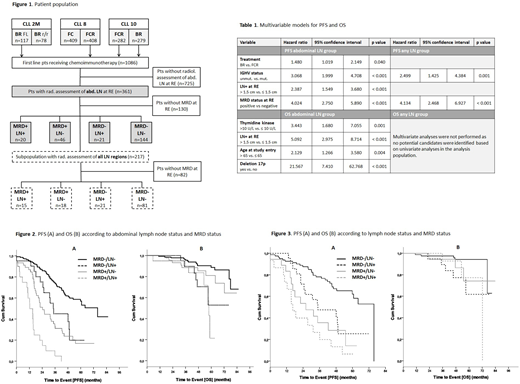
We included 361 pts receiving frontline CIT within 3 prospective clinical trials of the GCLLSG (CLL2M: 23 pts, CLL8: 113 pts, CLL10: 225 pts) with available CT/MRI scans to assess abdominal lymphadenopathy at the final restaging (FR; 2 months after the end of last treatment cycle). Pts with available data on all classical lymph node regions (N=217) were analyzed separately (Figure 1). Enlarged lymph nodes (LN+) were defined as >1.5 cm in the longest diameter according to iwCLL 2008 guidelines regardless of the investigator-assessed response category. MRD levels in peripheral blood (PB) were assessed at FR. PFS and OS was analyzed from time point of radiological assessment. Kaplan-Meier curves were plotted and compared using the log-rank test. Hazard ratios (HR) and 95% confidence intervals (CI) were calculated using Cox regression modelling.
Results:
Of the 361 pts included in this analysis, 227 (62.9%) received fludarabine, cyclophosphamide and rituximab (FCR) and 134 (37.1%) pts received bendamustine and R (BR). Median age was 60 years (range, 34-79); median observation time was 55.8 months (mo) (3.2-85.5).
62 (17.2%) pts had residual abdominal LN+, 299 (82.8%) had no residual abdominal lymphadenopathy (LN-) at FR. Of 217 pts with documented CT/MRI of all LN regions at FR, 48 (22.1%) pts had residual LN+ in at least one LN region and 169 (77.9%) showed no residual LN in any of the regions. Baseline characteristics were equally distributed between pts with and without available radiological assessments, between pts with radiological assessments of all regions or only abdominal and between LN+ and LN- pts. MRD in PB was available for 231 (64.0%) pts in this analysis group; of these, 165 pts (71.4%) showed MRD negativity (MRD-) at FR.
PFS and OS were analyzed for different LN size categories (≤1 cm; >1 & ≤2 cm; >2 & ≤3 cm; >3 cm). Patient outcome decreased with larger residual abdominal LN size at FR with regard to PFS (median, 52.9 mo vs. 24.6 mo vs. 30.5 mo vs. 10.6 mo; p<0.001) and OS (median, NR vs. 63.2 mo vs. 57.0 mo vs. 45.9 mo; p<0.001). However, the iwCLL guideline cut-off at 1.5 cm was found to be appropriate. Using this 1.5 cm cut-off, PFS and OS were significantly worse in abdominal LN+ pts compared to abdominal LN- pts (median PFS: 20.4 mo vs. 52.5 mo; HR 2.806; CI=2.030-3.879; p<0.001; median OS: 57 mo vs. not reached [NR]; HR 4.294; CI=2.600-7.091; p<0.001). In pts with residual lymphadenopathy >1.5 cm in any lymph node region, PFS and OS was significantly worse compared to LN- pts (median PFS: 27.3 mo vs. 60.4 mo; HR 2.409; CI=1.622-3.577; p<0.001; median OS: 60.7 mo vs. NR; HR 4.445; CI=2.208-8.947; p<0.001). In a multivariate analysis, abdominal LN size at FR was an independent prognostic factor for PFS and OS, while LN size in any lymph node region failed to show independent prognostic value (Table 1).
In the MRD- group, PFS was significantly shorter in MRD-/LN+ pts compared to MRD-/LN- pts (abdominal LN: median, 34.7 mo vs. 75.6 mo; HR 2.150; CI=1.190-3.883; p=0.011; any LN: median, 34.7 mo vs. 75.6 mo; HR 2.343; CI=1.221-4.497; p=0.01). This observation was confirmed for OS (abdominal LN: 5-year survival, 52.9% vs. 88.8%; HR 3.153; CI=1.183-8.407; p=0.022; any LN: 5-year survival, 61.9% vs. 94.3%; HR 4.213; CI=1.179-15.016; p=0.027) (Figures 2 & 3).
Conclusions:
Residual abdominal lymphadenopathy at FR is an independent prognostic factor for PFS and OS regardless of MRD negativity. It remains to be determined whether these findings can be transferred to novel targeted agents such as kinase inhibitors, venetoclax, novel CD20 antibodies or combinations of these. Residual disease in the lymph node compartment may identify a pt population which might benfit from strategies using consolidation therapies.
Bahlo:Roche: Honoraria, Other: Travel Grants. Fink:Celgene: Consultancy, Research Funding; AbbVie: Consultancy, Other: travel geants; Roche: Other: travel grants; Mundipharma: Other: travel grants. Dreyling:Roche: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria, Research Funding; Mundipharma: Consultancy, Research Funding; Bayer: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Sandoz: Consultancy; Acerta: Consultancy; Gilead: Consultancy, Honoraria. Hess:CTI: Research Funding; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Pfizer: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Consultancy, Honoraria, Other: travel expenses, Research Funding; Abbvie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees. Ritgen:Roche: Honoraria, Research Funding; abbvie: Research Funding. Kneba:AbbVie: Consultancy, Honoraria; Roche: Consultancy, Honoraria. Döhner:Bristol Myers Squibb: Research Funding; Jazz: Consultancy, Honoraria; Pfizer: Research Funding; Astellas: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Astex Pharmaceuticals: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Seattle Genetics: Consultancy, Honoraria; Astellas: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Celator: Consultancy, Honoraria; Pfizer: Research Funding; Amgen: Consultancy, Honoraria; AROG Pharmaceuticals: Research Funding; Agios: Consultancy, Honoraria; Sunesis: Consultancy, Honoraria, Research Funding; AROG Pharmaceuticals: Research Funding; AbbVie: Consultancy, Honoraria; Sunesis: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy, Honoraria; Seattle Genetics: Consultancy, Honoraria; Novartis: Consultancy, Honoraria, Research Funding; Novartis: Consultancy, Honoraria, Research Funding; Agios: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria; Jazz: Consultancy, Honoraria; Celator: Consultancy, Honoraria; Astex Pharmaceuticals: Consultancy, Honoraria; Bristol Myers Squibb: Research Funding. Stilgenbauer:AbbVie: Consultancy, Honoraria, Other: travel support, Research Funding; Roche: Consultancy, Honoraria, Other: travel support, Research Funding; Genetech: Consultancy, Honoraria, Other: travel support, Research Funding; Pharmacyclics: Consultancy, Honoraria, Other: travel support, Research Funding; Celgene: Consultancy, Honoraria, Other: travel support, Research Funding; Amgen: Consultancy, Honoraria, Other: travel support, Research Funding; GlaxoSmithKline: Consultancy, Honoraria, Other: travel support, Research Funding; Gilead: Consultancy, Honoraria, Other: travel support, Research Funding; Janssen: Consultancy, Honoraria, Other: travel support, Research Funding; Mundipharma: Consultancy, Honoraria, Other: travel support, Research Funding; Novartis: Consultancy, Honoraria, Other: travel support, Research Funding. Wendtner:Mundipharma: Consultancy, Honoraria, Research Funding; Pharmacyclics: Consultancy, Honoraria, Other: travel support, Research Funding; Gilead: Consultancy, Honoraria, Research Funding; GlaxoSmithKline: Consultancy, Honoraria, Other: travel support, Research Funding; Roche: Consultancy, Honoraria, Other: travel support, Research Funding; Abbvie: Consultancy, Honoraria, Other: travel support, Research Funding; Genetech: Consultancy, Honoraria, Other: travel support, Research Funding; Gilead: Consultancy, Honoraria, Other: travel support, Research Funding; Janssen: Consultancy, Honoraria, Other: travel support, Research Funding; MorphoSys: Consultancy, Honoraria, Other: travel support, Research Funding. Goede:Roche: Consultancy, Honoraria, Other: Travel grants; Janssen: Consultancy, Honoraria, Other: Travel grants; Gilead: Consultancy, Honoraria; AbbVie: Consultancy. Fischer:Roche: Other: Travel support. Böttcher:Genentech: Research Funding; Roche: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; AbbVie: Honoraria, Research Funding; Janssen: Honoraria; Celgene: Research Funding. Hallek:Janssen: Honoraria, Research Funding; Pharmacyclics: Honoraria, Research Funding; Abbvie: Honoraria, Research Funding; Roche: Honoraria, Research Funding; Celgene: Honoraria, Research Funding; Gilead: Honoraria, Research Funding; Mundipharma: Honoraria, Research Funding. Eichhorst:AbbVie, Celgene, Gilead, Janssen, Mundipharma, Novartis, Roche: Honoraria, Other: Travel support, Research Funding.

