

Background: Avatrombopag (AVA) is a novel, oral thrombopoietin receptor agonist (TPO-RA) recently FDA approved for the treatment of chronic immune thrombocytopenia (ITP) in patients who have not responded to prior therapies. Additionally, AVA is approved for the treatment of thrombocytopenia in chronic liver disease patients undergoing a procedure. AVA is unique in that it does not have a boxed safety warning for hepatoxicity, is administered with food, and does not have any dietary restrictions. Further, it does not interact with polyvalent cations (calcium, magnesium, iron, selenium, zinc, etc.) in foods, mineral supplements, or antacids that could reduce systemic exposure and efficacy.
Methods and Aims: A 6-month, multicenter, randomized, double-blind, Phase 3 study (Core Study) enrolled 32 AVA- and 17 placebo (PBO)-treated patients with ITP. The mean platelet count at Baseline was 13,600/µL for the study population. The starting dose for AVA was 20 mg QD, with subsequent dose titration (5 to 40 mg) to maintain platelet counts between 50,000 to 150,000/µL. The primary endpoint was the median cumulative number of weeks achieving a platelet count ≥50,000/µL, and AVA was shown to be superior to PBO (12.4 vs. 0.0 weeks, p<0.0001). Achieving a platelet count of ≥50,000/µL on Day 8 was a key secondary endpoint with 65.6% of AVA-treated patients meeting this endpoint versus 0% for PBO (p<0.0001). AVA had a favorable safety profile with the most frequently reported adverse events including headache, fatigue, contusion, epistaxis and upper respiratory tract infection. In addition, patients could enter the Extension Phase if they completed the 6-month Core Study, or if they experienced a lack of efficacy during that period.
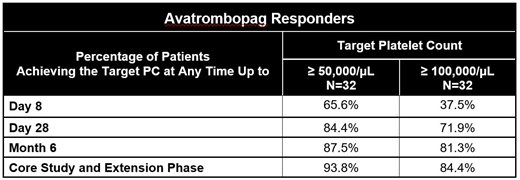
Reaching a target platelet count of ≥50,000/µL at any time is a common endpoint for therapies in clinical studies as well as in clinical practice, with a platelet count of ≥100,000/µL often being defined as a complete response. The objective of the analyses of these endpoints for the Phase 3 study was to provide previously unreported data, and further evaluate the efficacy of AVA in patients with ITP, i.e., the percentage of patients who achieved platelet counts ≥50,000/µL or ≥100,000/µL at any time during the Core Study and its Extension Phase.
Results: In the Core Study, a high proportion of AVA patients achieved a platelet count ≥50,000/µL relative to PBO by Day 28 (84.4% vs. 0.0%, respectively) and Week 26 (87.5% vs. 5.9%). In an integrated analysis of the Core Study and its Extension Phase, 93.8% of patients initially randomized to AVA achieved a platelet count of ≥50,000/µL at any time, and 64.7% of PBO patients who rolled-over to AVA in the Extension Phase also reached this metric. In addition, a high proportion of patients in the Core Study achieved platelet counts categorized as a complete response, with 81.3% of patients reaching a platelet count ≥100,000/µL at any time by Month 6, versus 5.9% with PBO. Across the Core Study and its Extension Phase, 84.4% of patients initially randomized to AVA and 58.8% of those who initially received PBO achieved a complete response at any time.
During the Extension Phase out through 36 weeks, both patients who were initially randomized to AVA and the PBO patients who rolled over to AVA in the Extension Phase maintained mean platelet counts ≥ 50,000/µL, demonstrating the consistency of efficacy for AVA; i.e., both PBO-treated patients responded to active drug and those previously administered AVA maintained platelet counts in the target range in the Extension Phase.
Conclusions: Analysis of these previously unreported alternative efficacy endpoints that are standard across other clinical studies demonstrated a high proportion of AVA-treated patients in the Phase 3 study as responders or complete responders. Further, the integrated analyses of the Phase 3 Core Study and Extension Phase data provides additional information regarding the durability of the AVA response, and illustrates the consistency of effect with PBO-treated patients also responding to subsequent treatment with AVA.
Nagalla:Alnylam: Membership on an entity's Board of Directors or advisory committees. Vredenburg:Dova Pharmaceuticals: Employment, Other: Shareholder. Allen:Dova Pharmaceuticals: Equity Ownership, Other: Chief Medical Officer .

