

Background: Double filtration plasmapheresis (DFPP) is a form of therapeutic plasma exchange (TPE) that removes high-molecular-weight (HMW) pathological mediators from the plasma with two filters: a plasma separator and a plasma fractionator. Relative to simple TPE, the semi-selectiveness of DFPP reduces protein loss and the need for substitution fluid. However, depending on the choice of plasma fractionator, DFPP may negatively impact hemostatic components such as HMW coagulation factors.
Aim: To determine the impact of DFPP on various hemostatic parameters (i.e. FVIII activity, fibrinogen level, vWF level and activity, ADAMTS13 level and activity, protein C (PC) activity, protein S (PS) activity, antithrombin (AT) activity, prothrombin time (PT), and activated partial thromboplastin time (aPTT)).
Methods: Fourteen patients undergoing weekly, bimonthly, or monthly DFPP sessions for hematologic conditions (n=11) or nervous system disorders (n=3) were recruited. Hemostatic parameters were measured immediately before and after 27 DFPP sessions (1-4 sessions/patient). The treatment volume was standardized at one plasma volume, and anticoagulation was performed with ACD-A citrate dextrose solution. EC-30W and EC-50W were used as the plasma fractionators in 4 and 23 sessions, respectively.
In addition to primary data collection, we systematically searched PubMed, MEDLINE, and EMBASE for studies that investigated the impact of DFPP on hemostasis. No restriction was placed on filter choice.
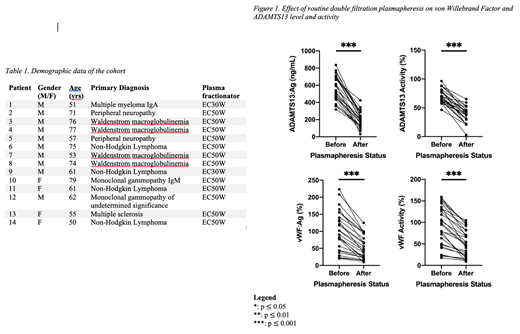
Results: In our cohort of 14 patients, all hemostatic changes were statistically significant. After a routine DFPP session, the level and/or activity of HMW proteins (>100kDa: FVIII, fibrinogen, vWF, ADAMTS13) were decreased more than those of low-molecular-weight (LMW) proteins (<100kDa: PC, PS, AT). Mean pre- vs post-DFPP values are reported in brackets beside the corresponding parameter. FVIII activity (99.9% s.d. 49.2% vs 54.2% s.d. 33.4%; p<0.0001) and fibrinogen level (325mg/dL s.d. 112mg/dL vs 168mg/dL s.d. 71.1mg/dL; p<0.0001) were decreased by 45 s.d. 16% and 49 s.d. 13% compared to baseline, respectively. vWF level (99.3% s.d. 57.6% vs 52.2% s.d. 34.2%; p<0.0001) and activity (90.4% s.d. 46.1% vs 51.1% s.d. 31.6%; p<0.0001) were decreased by 46 s.d. 20% and 43 s.d. 17% relative to baseline, respectively. ADAMTS13 level (556ng/mL s.d. 142ng/mL vs 204ng/mL s.d. 89.8ng/mL; p<0.0001) and activity (70.1% s.d. 13.1% vs 38.3% s.d. 14%; p<0.0001) were decreased by 63 s.d. 13% and 44 s.d. 22% compared to baseline, respectively. Contrasting the 43-63% reductions of HMW proteins from baseline, PC activity (98.9% s.d. 22.9% vs 72.3% s.d. 22.3%; p<0.0001), PS activity (64.3% s.d. 13.2% vs 45.4% s.d. 13%; p<0.0001), and AT activity (100% s.d. 18.5% vs 74.8% s.d. 19.9%; p<0.0001) were decreased by 26 s.d. 17%, 29 s.d. 15%, and 25 s.d. 16%, respectively. In terms of coagulation tests, PT expressed as an internalized normalized ratio (1.07 s.d. 0.174 vs 1.43 s.d. 0.737; p=0.0005) increased by 35 s.d. 71%, whereas PT expressed as a percentage (94.2% s.d. 22.3% vs 68.2% s.d. 14.5%; p<0.0001) decreased by 25 s.d. 16% relative to baseline. Furthermore, aPTT expressed in seconds (35s s.d. 6.63s vs 47.1s s.d. 31.9s; p=0.0074) and as a ratio (1 s.d. 0.189 vs 1.35 s.d. 0.917; p=0.008) increased by 36 s.d. 94% and 36 s.d. 95% compared to baseline, respectively.
Our systematic review included 26 cohort studies, 6 case reports, and 1 randomized controlled trial. Increases in INR and aPTT following DFPP were considerably higher in previous studies, which may relate to the commonality of heparin-induced anticoagulation. The present study is the first comprehensive investigation of the impact of DFPP on hemostatic parameters with such a large sample size. It is also the first study of its nature to measure ADAMTS13-related parameters.
Conclusions: Routine DFPP resulted in significant reduction across all investigated hemostatic proteins and significant prolongation of clotting tests. The activities of HMW coagulation-related proteins were decreased more than those of LMW anticoagulation-related proteins. This finding suggests that DFPP may increase overall bleeding risk, a consideration for patient safety that may be of importance in continuous DFPP treatment. Additional high quality evidence is needed to elucidate the effect of DFPP on the hemostatic system.
Matino:Sanofi: Honoraria; Sobi: Honoraria, Research Funding; Roche: Research Funding; Bayer: Honoraria, Research Funding; Pfizer: Honoraria, Research Funding; Bioviiix: Honoraria.

