

Background:Patients with clonal hematopoiesis (CH) in the absence of WHO-classified myeloid disease are of special interest given their increased prevalence with age, predisposition to morbid cardiovascular complications, and amplified risk of overt hematologic malignancy. Pts are often stratified by normal peripheral blood counts into clonal hematopoiesis of indeterminate potential (CHIP), or those with unexplained cytopenias as clonal cytopenias of undetermined significance (CCUS). However, less is known about pts with elevated counts and clonal hematopoiesis who do not fulfill WHO criteria for any myeloproliferative neoplasia (MPN). We leveraged Vanderbilt University Medical Center's unique biobank, BioVU, to identify the prevalence of JAK2V617Facross 48,000 pts to evaluate the clinical changes in progression from CH to overt myeloid disease.
Methods:To develop a reference JAKV617Ftraining set, next generation sequencing via Illumina Trusight Myeloid Panel (NGS) was performed on BioVU samples (N=133) from pts with confirmed myeloproliferative malignancy. Of those pts, 78 harbored JAK2V617Fwith a range of variant allele frequencies (VAF). Matched samples in this training set (N=133) were also analyzed via Infinium® Expanded Multi-Ethnic Genotyping Array (MEGAEX). SNP array JAK2V617Fvariant intensity was extracted (rs77375493; NM_004972.3(JAK2): c.1849G>T (p.Val617Phe). A regression model was built using NGS VAF as a dependent variable and MEGAEX intensity data as independent variable (r2=0.9931).Based on this model, we imputed JAK2V617FVAF for all 48,000 pts in our cohort.
Pts with JAK2V617Fwere subdivided into: clinically confirmed myeloid disease, or JAK2V617Fwithout a diagnosis of MPN. Upon review of the EMR, the latter group was further dived into: 1) probable undiagnosedMPN, 2) CHIP, 3) CCUS, or 4) CH with associated elevated peripheral blood counts (CHAPbc). Only lab values after the date of JAK2V617Fdetection were included. Confirmed malignancy was defined by WHO classification of disease. Pts with evidence of possible WHO classified PV or ET with Hgb >18.5g/dl in men, >16.5g/dl in women, or PLT count >450k/mcl regardless of gender were classified as probable undiagnosedMPN. CHIP was defined as JAK2V617Fwithout abnormal counts across a patient's EMR lifetime, except when confounding events, e.g. trauma surgery or overt iron deficiency anemia, incorrectly skewed values. CCUS was defined as JAK2V617Fin the presence of unexplained cytopenias; hemoglobin (Hgb) <13.5g/dl men or <12g/dl women, leukocyte count (WBC) <3.9x10^3/uL or platelet (PLT) <135 x10^3/mcL. We classified pts with elevated blood counts who did not meet the WHO classification of MPN [e.g. WBC >10.7 regardless of gender, Hgb 18-18.5 g/dL in men or 16.0-16.5 g/dL in women with maximum Hgb no greater than 18.5g/dl in men and 16.5g/dl in women, or PLT count between 371-450k/mcl regardless of gender (and no values >450k/mcl)] as CHAPbc.
Results:We identified 410 of 48,000 pts who harbored JAK2V617F(0.85% prevalence). Of those, 270/410 had clinically diagnosed hematologic malignancy including primary myelofibrosis (PMF) (79), ET (48), PV (43) and Ph-MPN NOS (29). MDS (29), AML (15), NHL (16), plasma cell dyscrasias (5), CML (3), other (3). There were 19/410 with insufficient clinical data to determine diagnosis.
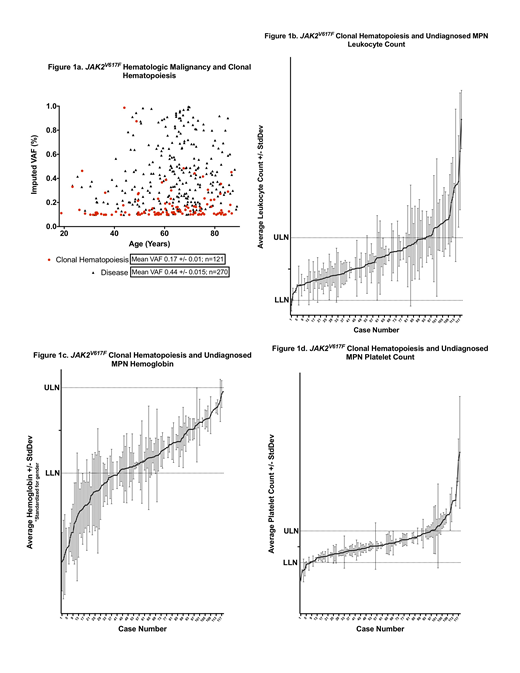
The remaining 121/410 JAK2V617Fpts did not have a related diagnosis. Figure 1a demonstrates imputed VAF differences in JAK2V617Fbetween known MPN vs. CH (including undiagnosed MPN) by age (mean VAF 0.44 vs. 0.17 respectively P<0.001). We identified several undiagnosed MPNs (22), which subdivided into polycythemia predominant (1), thrombocythemia predominant (16) or a combination of polycythemia and thrombocythemia (5). The remaining 99/410 cases were CH,with CHIP (55), CCUS (29), and CHAPbc (15). Ranges of blood counts appear to be a continuous variable among JAK2V617Fpts with CH or undiagnosed MPN (Fig 1b-1d).
Summary: We used an unbiased approach to identify the prevalence of JAK2V617Facross all pts at a single institution. In this cohort, hematologic malignancy and CH did stratify by imputed VAF. Further, within JAK2V617FCH, CHAPbc may be differentiated from CHIP by clinical phenotype and further investigation will be required to determine its impact on patient outcomes.
Savona:Sunesis: Research Funding; TG Therapeutics: Membership on an entity's Board of Directors or advisory committees, Research Funding; Incyte Corporation: Membership on an entity's Board of Directors or advisory committees, Research Funding; AbbVie: Membership on an entity's Board of Directors or advisory committees; Boehringer Ingelheim: Patents & Royalties; Selvita: Membership on an entity's Board of Directors or advisory committees; Karyopharm Therapeutics: Consultancy, Equity Ownership, Membership on an entity's Board of Directors or advisory committees; Celgene Corporation: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees, Research Funding.

