


Introduction: t-AML is generally defined as AML arising from prior cytotoxic therapy, ionizing radiotherapy, or immunotherapy for an unrelated disease and is associated with poorer outcomes relative to de novo AML, with a median overall survival (OS) of ~6 mo following conventional induction chemotherapy. CPX-351 (Vyxeos®; daunorubicin and cytarabine liposome for injection) is a dual-drug liposomal encapsulation of cytarabine [C] and daunorubicin [D] at a synergistic 5:1 molar ratio. In a phase 3 study (NCT01696084) in older patients (pts) with newly diagnosed, high-risk/secondary AML, induction followed by consolidation with CPX-351 significantly improved OS (9.56 vs 5.95 mo; hazard ratio [HR] = 0.69; 1-sided P = 0.003) vs conventional 7+3, with a comparable safety profile. CPX-351 is approved by the FDA and EMA for the treatment of adults with newly diagnosed t-AML or AML with myelodysplasia-related changes. An exploratory analysis of the phase 3 study was performed to compare outcomes in the subgroup of pts with t-AML who achieved complete remission (CR) or CR with incomplete neutrophil or platelet recovery (CRi).
Methods: Pts aged 60-75 y with newly diagnosed, high-risk/secondary AML were randomized 1:1 to receive 1-2 induction cycles with CPX-351 (100 units/m2 [C 100 mg/m2 +D 44 mg/m2] as a 90-min infusion on Days 1, 3, and 5 [2nd induction: Days 1 and 3]) or 7+3 (C 100 mg/m2/day continuously for 7 d [2nd induction: 5 d] + D 60 mg/m2 on Days 1-3 [2nd induction: Days 1-2]). Pts achieving CR+CRi could receive up to 2 consolidation cycles with CPX-351 (65 units/m2 [C 65 mg/m2 + D 29 mg/m2] on Days 1 and 3) or 5+2 (as in 2nd induction). Pts could receive hematopoietic cell transplantation (HCT) at the physician's discretion. This exploratory analysis compared outcomes for CPX-351 vs 7+3 in the subgroup of t-AML pts who achieved CR+CRi.
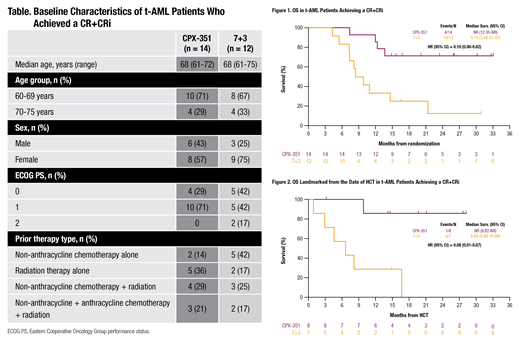
Results: Of 309 enrolled pts, 63 (20%) were diagnosed with t-AML. Among t-AML pts, 14/30 (47%) receiving CPX-351 and 12/33 (36%) receiving 7+3 achieved a CR+CRi (odds ratio = 1.53 [95% CI: 0.56-4.20]). Fewer pts treated with CPX-351 vs 7+3 received prior treatment with non-anthracycline chemotherapy alone (CPX-351: 14%; 7+3: 42%) whereas prior radiation therapy alone was less frequent in 7+3 pts (36%; 17%). Prior exposure to non-anthracycline chemotherapy with radiation (29%; 25%) and non-anthracycline chemotherapy with anthracycline chemotherapy and radiation (21%; 17%), as well as other baseline characteristics, were balanced between arms (Table).
Median OS was longer with CPX-351 vs 7+3 in t-AML pts who achieved a CR+CRi (not reached [NR] vs 9.15 mo; HR = 0.19 [95% CI: 0.06-0.62]; Figure 1). While the rate of HCT in pts with CR+CRi was similar with CPX-351 and 7+3 (57% vs 58%; relative risk = 0.97 [95% CI: 0.50-1.90]), OS landmarked from the HCT date was longer with CPX-351 (NR vs 6.60 mo; HR = 0.08 [95% CI: 0.01-0.67]; Figure 2). No pt relapsed prior to HCT. Additional antileukemia therapy was received during follow-up prior to HCT by 7/8 (88%) pts in the CPX-351 arm and 7/7 (100%) pts in the 7+3 arm. Median OS in CR+CRi pts who did not receive a HCT was NR (95% CI: 7.43-NR) with CPX-351 vs 8.48 mo (95% CI: 5.49-NR) with 7+3.
The most common treatment-emergent adverse events (TEAEs) in t-AML pts who achieved CR+CRi were febrile neutropenia (CPX-351: 100%; 7+3: 67%), rash (64%; 25%), epistaxis (57%; 25%), nausea (50%; 67%), diarrhea (43%; 67%), decreased appetite (43%; 58%), chills (29%; 50%), and fatigue (21%; 50%). A cardiac TEAE occurred in 4 (29%) pts in the CPX-351 arm and 4 (33%) pts in the 7+3 arm; the most common cardiac TEAEs were mitral valve incompetence (14%; 0%) and atrial fibrillation (7%; 17%). The most common grade ≥3 TEAEs were febrile neutropenia (CPX-351: 93%; 7+3: 67%), pneumonia (21%; 8%), and bacteremia (21%; 0%). The most common serious TEAEs were febrile neutropenia (CPX-351: 43%; 7+3: 0%), cellulitis (14%; 0%), and syncope (14%; 0%). There was no early mortality by Day 60 in either arm for t-AML pts who achieved a CR+CRi.
Conclusions: Among t-AML pts who achieved a CR+CRi, CPX-351 improved median OS and OS landmarked from the HCT date vs 7+3 chemotherapy. Differences in outcomes may have been influenced by fewer pts treated with 7+3 who received prior radiation therapy only. The safety profile for CPX-351 in this subgroup was generally consistent with the known profile of 7+3. Exploratory analyses of baseline and post-treatment molecular (mutational) characteristics is ongoing.
Lancet:Agios, Biopath, Biosight, Boehringer Inglheim, Celator, Celgene, Janssen, Jazz Pharmaceuticals, Karyopharm, Novartis: Consultancy; Pfizer: Consultancy, Research Funding; Daiichi Sankyo: Consultancy, Other: fees for non-CME/CE services . Rizzieri:Spectrum: Consultancy; AbbVie: Consultancy; TEVA: Consultancy; Millennium: Speakers Bureau; Amgen: Consultancy; Novartis: Consultancy; Kite Pharma: Consultancy; Gilead Sciences: Consultancy, Speakers Bureau; Incyte: Consultancy, Speakers Bureau; Pfizer: Consultancy; Seattle Genetics: Consultancy, Speakers Bureau; Jazz Pharmaceuticals: Speakers Bureau. Schiller:Genzyme: Research Funding; Gilead: Research Funding; Incyte: Research Funding; J&J: Research Funding; Jazz Pharmaceuticals: Honoraria, Research Funding; Karyopharm: Research Funding; Novartis: Research Funding; Onconova: Research Funding; Pfizer Pharmaceuticals: Equity Ownership, Research Funding; Sangamo Therapeutics: Research Funding; Agios: Research Funding, Speakers Bureau; Amgen: Other, Research Funding; Astellas: Research Funding; Biomed Valley Discoveries: Research Funding; Bristol Myer Squibb: Research Funding; Celgene: Research Funding, Speakers Bureau; Constellation Pharmaceutical: Research Funding; Daiichi Sankyo: Research Funding; Eli Lilly and Company: Research Funding; FujiFilm: Research Funding. Erba:Amgen, Celgene, Daiichi Sankyo, ImmunoGen, Incyte, Jazz Pharmaceuticals, Millennium, Novartis, Ono, Pfizer, Seattle Genetics, Sunesis: Consultancy; Celgene, Incyte, Novartis: Speakers Bureau; Agios, Amgen, Astellas Pharma, Daiichi Sankyo, ImmunoGen, Janssen, Jazz Pharmaceuticals, Juno, Millennium, Seattle Genetics: Research Funding. Ryan:Jazz Pharmaceuticals: Employment, Equity Ownership. Faderl:Jazz Pharmaceutics: Employment, Equity Ownership. Cortes:Sun Pharma: Research Funding; Jazz Pharmaceuticals: Consultancy, Research Funding; Forma Therapeutics: Consultancy, Honoraria, Research Funding; Pfizer: Consultancy, Honoraria, Research Funding; Astellas Pharma: Consultancy, Honoraria, Research Funding; BiolineRx: Consultancy; Merus: Consultancy, Honoraria, Research Funding; Immunogen: Consultancy, Honoraria, Research Funding; Biopath Holdings: Consultancy, Honoraria; Bristol-Myers Squibb: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; Novartis: Consultancy, Honoraria, Research Funding; Daiichi Sankyo: Consultancy, Honoraria, Research Funding.
This icon denotes a clinically relevant abstract

