

Background: The normal function of isocitrate dehydrogenase 1 (IDH1) is to catalyze the conversion of cytoplasmic isocitrate to α-ketoglutarate (aKG) in the Krebs cycle. In hematologic malignancies a hotspot mutation at arginine 132 within the conserved active site of IDH1 leads to loss of the expected Krebs Cycle reaction as well as production of the oncometabolite 2- hydroxyglutarate (2-HG). In acute myeloid leukemia (AML) increased cellular 2-HG levels has been shown to impact the tumor microenvironment and promotes tumorigenesis via paracrine stimulation as well repression of the tumor associated immune system. Ivosidenib (AG-120) is a small molecule inhibitor of mIDH1 and is FDA approved for the treatment of patients (pts) with relapsed refractory IDH1 mutant AML. Ivosidenib is known to lower 2-HG levels, independent of response. By reducing 2-HG levels that promote immune escape of IDH-mutant tumors with ivosidenib, we hope to harness the known programmed death receptor pathway dysregulation in AML and high risk myelodysplastic syndrome (MDS).
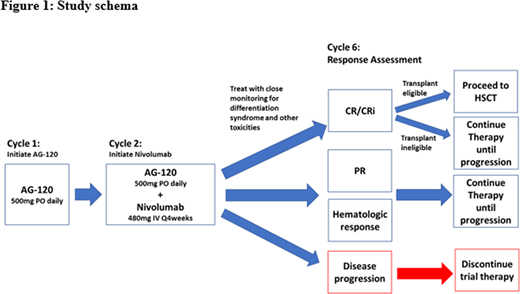
Study Design and Methods: IVO-NIVO is a single arm, multi-institutional phase II investigator initiated clinical trial with a safety cohort to confirm safety and tolerability of combination AG-120 and nivolumab. To be included pts must have MDS or AML with a documented IDH1 mutation in blood or bone marrow within 30 days of inclusion based on mutational testing by PCR or sequencing in a CLIA certified laboratory and be willing to undergo a bone marrow biopsy. Pts will initially start therapy with AG-120, 500mg by mouth daily for 1 cycle. A cycle is defined as 28 days of therapy. On cycle 2 day 1 enrolled pts will receive nivolumab 480 mg that will subsequently be infused every four weeks. Disease response to treatment will be serially assessed through the evaluation of blood (at least monthly) and bone marrow biopsies and aspirates. A complete response assessment will be performed after 6 cycles of therapy. Transplant eligible pts may proceed to allogeneic stem cell transplant (ASCT) if complete response (CR) or morphologic complete remission with incomplete count recovery (CRi) is achieved. Pts that are not eligible for ASCT will continue to receive AG-120- nivolumab combination therapy until documented progression or unacceptable toxicity (figure 1).
Safety Cohort: We will have an interim safety analysis after the first 6 pts finishing the first cycle of combination therapy to ensure dosing is safe and tolerable. Pts will undergo clinical assessment with each cycle of therapy, with particular attention to known toxicities like differentiation syndrome that may be life threatening. If 0 to 1 of the first 6 subjects experienced unacceptable toxicities the study will continue as planned. If 2 pts experienced unacceptable toxicities, accrual will be temporarily suspended in order to conduct a review of safety data. If after review, a safety issue is identified and can be corrected, the protocol will be amended accordingly, and enrollment will restart. If an additional 2 pts (4 of 12) or more experience an unacceptable toxicity the patient will be taken off trial and the trial will be terminated.
Statistical plan: It is estimated that 45 pts will be enrolled on trial. Using optimal Simon Stage 2 minimax design, if less than 7 of the first 16 pts respond the treatment will be study will be stopped for futility (type 1 error 0.05, type 2 error 0.2).
Primary endpoint: We aim to improve the cumulative response rate after 6 cycles of therapy from 40% to 60% (Two-sided alpha risk of 0.05, 1-Beta of 0.8 = 38 pts + 7 additional pts for potential drop-off observed in prior studies) in pts with mIDH1 relapsed/ refractory AML and MDS. Based on published data, it is known that overall response rate is approximately 40% to single agent AG-120 in the relapsed/ refractory IDH1 mutant AML population. Therefore, we expect a 20% ORR improvement compared to historical control after 6 cycles of treatment, based on MDS International Working Group 2006 criteria and AML MDS International Working group MDS/AML criteria.
Secondary endpoints: Progression-free survival (the interval between the time of initiation of olaparib to the time of documentation of olaparib failure or last follow-up), overall survival (the interval between the time of initiation of olaparib to the time of death or last follow-up) and percentage of pts that can be bridged to ASCT.
Prebet:novartis: Honoraria; Jazz Pharmaceuticals: Consultancy, Honoraria, Research Funding; pfizer: Honoraria; Bristol-Myers Squibb: Honoraria, Research Funding; Boehringer Ingelheim: Research Funding; Genentech: Consultancy; novartis: Honoraria; pfizer: Honoraria; novartis: Honoraria; Boehringer Ingelheim: Research Funding; novartis: Honoraria; pfizer: Honoraria; pfizer: Honoraria; Tetraphase: Consultancy; Agios: Consultancy, Research Funding; pfizer: Honoraria; novartis: Honoraria; Boehringer Ingelheim: Research Funding.
We will use Ivosidenib and nivolumab in combination as a part of a clinical trial to improve care of patients with relapsed/ refractory AML and MDS

