

Introduction
Primary bone diffuse large B-cell lymphoma (PB-DLBCL) is a rare extranodal lymphoma comprising 1-2% of all malignant lymphomas. This study aims to elucidate the genetic background of a homogeneous cohort of PB-DLBCL.
Methods
This retrospective study consists of primary DLBCL-patients with bone localization(s) of which pretreatment fresh frozen or formalin-fixed paraffin-embedded bone tissue samples were available. Patients were diagnosed (2003-2019) at Leiden University Medical Center (LUMC), a center of expertise for bone tumors, Amsterdam University Medical Center (AUMC), Erasmus MC and affiliated Dutch hospitals. Based on strict definitions regarding radiological assessment of anatomical disease localizations at diagnosis three subgroups were categorized: solely osseous involvement (single or multiple bone lesions; PB-DLBCL), osseous involvement and locoregional lymphadenopathy (locoregional disease), and osseous and (multiple) extra-osseous localizations (disseminated disease).
Cell-of-origin (COO) was determined by immunohistochemistry (BCL6, CD10, and MUM1) and classified according to the Hans' algorithm. Additionally, COO was confirmed with NanoString and the Lymph2Cx assay (Scott et al., Blood 2014), in a subset of patients.
With similar procedures (Vermaat et al., Haematologica 2019), molecular profiles were determined with an in-house developed and validated targeted next-generation sequencing (tNGS) panel, comprising 52 DLBCL-specific genes, for sequencing with the Ion S5TM System. Obtained results were compared to sequencing data of (1) an independent 'in-house' cohort of 23 primary GCB (Germinal Center B-Cell)-DLBCL patients without bone localization ('non-osseous') and (2) pooled data of 651 GCB-DLBCL patients from literature (Chapuy et al., Nature Medicine 2018, Karube et al., Leukemia 2018, Reddy et al., Cell 2017, Schmitz et al., NEJM 2018).
Results
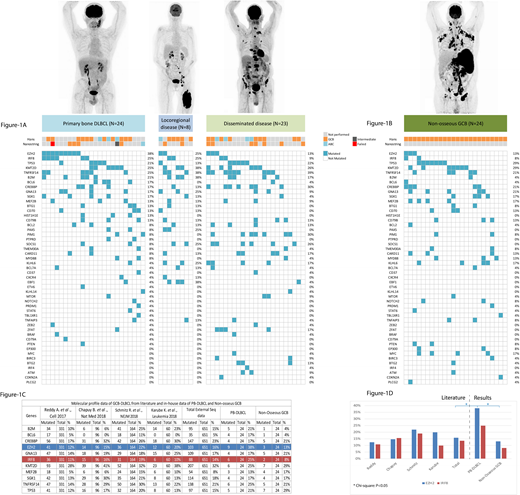
Our cohort contained 56 patients (males, N=33, (59%)) with a median age at diagnosis of 62 years (range 13-92). Twenty-four patients had PB-DLBCL (45%), 8 had locoregional disease (14%), and 23 had disseminated disease (41%). In general, immunohistochemistry and Lymph2Cx identified a GCB subtype for the majority of all DLBCL with bone localizations (Figure-1A) and these results for the hitherto unperformed cases will follow shortly.
tNGS identified 48 genes with 'pathogenic' mutations, with on average four mutated genes per patients (range 0-10; Figure-1A). Overall, high mutation frequencies were observed in TNFRSF14 (33%), KMT2D (27%), EZH2 (25%), CREBBP (22%), B2M (22%), and TP53 (20%) in DLBCL with bone localizations and mainly genes involved in epigenetic machinery. In PB-DLBCLs, high frequency of mutated EZH2 (38%) and IRF8 (25%) were identified. Both are epigenetic genes that regulates tumor suppression and type I interferon, respectively. In four PB-DLBCLs EZH2 and IRF8 were concomitantly mutated. Locoregional disease showed a similar molecular profile as PB-DLBCL. Association with clinical characteristics will be performed shortly.
Compared to our cohort of non-osseous GCB-DLBCL (Figure-1B) and pooled data of GCB-DLBCL in large sequencing studies (Figure-1C), EZH2 (Chi-square; P=0.046 and P=0.005, respectively) was significantly more frequently mutated in PB-DLBCL, though IRF8 did not attain this significance (Chi-square; P=0.121 and P=0.111, respectively; Figure-1D).
Conclusion
This study is the first that provides integrative analyses of immunohistochemistry, Lymph2Cx, and tNGS of a homogeneous cohort of PB-DLBCL, demonstrating the importance of epigenetic genes in lymphomagenesis. In contrast to (non-osseous) GCB-DLBCLs, the molecular profile of PB-DLBCL is characterized by significantly frequent mutations in EZH2 and frequent mutations in IRF8 and other epigenetic genes, which is indicative for a GCB phenotype (Scherer F. et al., Sci Transl Med 2016) and supported by immunohistochemistry and Lymph2Cx data. These results suggest that PB-DLBCL is a specific DLBCL-entity with a unique molecular profile and provide a rationale for exploration of novel targeted treatment with EZH2 (and IRF8) inhibitors for PB-DLBCL patients.
Lugtenburg:Genmab: Consultancy, Honoraria; Servier: Consultancy, Honoraria, Research Funding; Roche: Consultancy, Honoraria, Research Funding, Speakers Bureau; BMS: Consultancy; Celgene: Consultancy, Honoraria; Janssen Cilag: Honoraria; Takeda: Consultancy, Honoraria, Research Funding. Kersten:Gilead: Honoraria; Mundipharma: Honoraria, Research Funding; Roche: Honoraria, Research Funding; Celgene: Honoraria, Research Funding; Amgen: Honoraria, Research Funding; Takeda Oncology: Research Funding; Miltenyi: Honoraria; Kite Pharma: Honoraria, Research Funding; Bristol-Myers Squibb: Honoraria, Research Funding; Novartis: Honoraria.

