

Introduction: The R-MegaCHOEP trial showed that dose-escalation of conventional chemotherapy necessitating autologous stem cell transplantation (ASCT) does not confer a survival benefit for younger patients (pts) with high-risk aggressive B-cell lymphoma in the Rituximab era (Schmitz et al., Lancet Oncology 2012; 13, 1250-1259). To describe efficacy and toxicity over time and document the long-term risks of relapse and secondary malignancy we present the 10-year follow-up of this study.
Methods: In the randomized, prospective phase 3 trial R-MegaCHOEP younger pts aged 18-60 years with newly diagnosed, high-risk (aaIPI 2-3) aggressive B-cell lymphoma were assigned to 8 cycles of CHOEP (cyclophosphamide, doxorubcine, vincristine, etoposide, prednisone) or 4 cycles of dose-escalated high-dose therapy (HDT) necessitating repetitive ASCT both combined with Rituximab. Both arms were stratified according to aaIPI, bulky disease, and center. Primary endpoint was event-free survival (EFS). All analyses were calculated for the intention-to-treat population. This follow-up report includes molecular data based on immunohistochemistry (IHC) and fluorescent in situ hybridization (FISH) for MYC (IHC: 31/92 positive [40-100%], FISH: 14/103 positive), BCL2 (IHC: 65/89 positive [50-100%], FISH: 23/111 positive) and BCL6 (IHC: 52/86 positive [30-100%], FISH: 34/110 positive) and data on cell of origin (COO) classification according to the Lymph2CX assay (GCB: 53/88; ABC: 24/88; unclassified: 11/88).
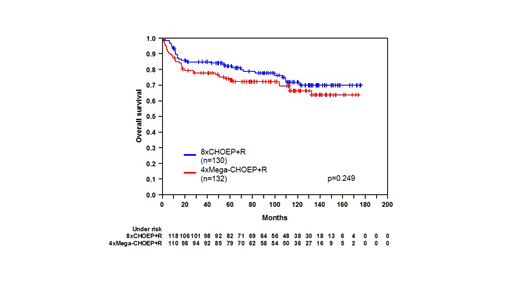
Results: 130 pts had been assigned to R-CHOEP and 132 to R-MegaCHOEP. DLBCL was the most common lymphoma subtype (~80%). 73% of pts scored an aaIPI of 2 and 27% an aaIPI of 3. 60% of pts had an initial lymphoma bulk and in 40% more than 1 extranodal site was involved. After a median observation time of 111 months, EFS at 10 years was 57% (95% CI 47-67%) in the R-CHOEP vs. 51% in the R-MegaCHOEP arm (42-61%) (hazard ratio 1.3, 95% CI 0.9-1.8, p=0.228), overall survival (OS) after 10 years was 72% (63-81%) vs. 66% (57-76%) respectively (p=0.249). With regard to molecular characterization, we were unable to detect a significant benefit for HDT/ASCT in any subgroup analyzed. In total, 16% of pts (30 pts) relapsed after having achieved a complete remission (CR). 23% of all relapses (7 pts) showed an indolent histology (follicular lymphoma grade 1-3a) and 6 of these pts survived long-term. In contrast, of 23 pts (77%) relapsing with aggressive DLBCL or unknown histology 18 pts died due to lymphoma or related therapy. The majority of relapses occurred during the first 3 years after randomization (median time: 22 months) while after 5 years we detected relapses only in 5 pts (3% of all 190 pts prior CR). 11% of pts were initially progressive (28 pts) among whom 71% (20 pts) died rapidly due to lymphoma. Interestingly, the remaining 29% (8 pts) showed a long-term survival after salvage therapy (+/- ASCT); only 1 pt received allogeneic transplantation. The frequency of secondary malignancies was very similar in both treatment arms (9% vs. 8%) despite the very high dose of etoposide (total 4g/m2)in the R-MegaCHOEP arm. We observed 2 cases of AML and 1 case of MDS per arm. In total 70 pts (28%) have died: 30 pts due to lymphoma (12%), 22 pts therapy-related (11 pts due to salvage therapy) (9%), 8 pts of secondary neoplasia (3%), 5 pts due to concomitant disease (2%) and 5 pts for unknown reasons.
Conclusions: This 10-year long-term follow-up of the R-MegaCHOEP trial confirms the very encouraging outcome of young high-risk pts following conventional chemotherapy with R-CHOEP. High-dose therapy did not improve outcome in any subgroup analysis including molecular high-risk groups. Relapse rate was generally low. Pts with aggressive relapse showed a very poor long-term outcome while pts with indolent histology at relapse survived long-term. Secondary malignancies occurred; however, they were rare with no excess leukemias/MDS following treatment with very high doses of etoposide and other cytotoxic agents.
Supported by Deutsche Krebshilfe.
Nickelsen:Roche Pharma AG: Membership on an entity's Board of Directors or advisory committees, Other: Travel Grants; Celgene: Membership on an entity's Board of Directors or advisory committees, Other: Travel Grant; Janssen: Membership on an entity's Board of Directors or advisory committees. Hänel:Amgen: Honoraria; Celgene: Other: advisory board; Novartis: Honoraria; Takeda: Other: advisory board; Roche: Honoraria. Truemper:Nordic Nanovector: Consultancy; Roche: Research Funding; Mundipharma: Research Funding; Janssen Oncology: Consultancy; Takeda: Consultancy, Research Funding; Seattle Genetics, Inc.: Research Funding. Held:Roche: Consultancy, Other: Travel support, Research Funding; Amgen: Research Funding; Acrotech: Research Funding; MSD: Consultancy; Bristol-Myers Squibb: Consultancy, Other: Travel support, Research Funding. Dreyling:Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: scientific advisory board, Research Funding, Speakers Bureau; Bayer: Consultancy, Other: scientific advisory board, Speakers Bureau; Celgene: Consultancy, Other: scientific advisory board, Research Funding, Speakers Bureau; Mundipharma: Consultancy, Research Funding; Gilead: Consultancy, Other: scientific advisory board, Speakers Bureau; Novartis: Other: scientific advisory board; Sandoz: Other: scientific advisory board; Janssen: Consultancy, Other: scientific advisory board, Research Funding, Speakers Bureau; Acerta: Other: scientific advisory board. Viardot:Kite/Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Honoraria; F. Hoffmann-La Roche Ltd: Honoraria, Membership on an entity's Board of Directors or advisory committees. Rosenwald:MorphoSys: Consultancy. Lenz:Gilead: Consultancy, Honoraria, Research Funding, Speakers Bureau; AstraZeneca: Consultancy, Honoraria, Research Funding; Agios: Research Funding; Celgene: Consultancy, Honoraria, Research Funding, Speakers Bureau; Bayer: Consultancy, Honoraria, Research Funding, Speakers Bureau; Janssen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Roche: Employment, Honoraria, Research Funding, Speakers Bureau; BMS: Consultancy. Schmitz:Novartis: Honoraria; Gilead: Honoraria; Celgene: Equity Ownership; Riemser: Consultancy, Honoraria.

