

Introduction:
Chronic liver disease (CLD) results in thrombocytopenia [1]. Depression of thrombopoietin (TPO) levels in CLD leads to thrombocytopenia. Thrombocytopenia increases the risk of bleeding in patients undergoing invasive diagnostic or therapeutic procedures [2]. TPO agonists have been depicted to be safe and efficacious in the treatment of thrombocytopenia due to idiopathic immune thrombocytopenia and aplastic anemia. Several studies have evaluated the use of TPO agonist versus placebo for pre-procedural treatment of thrombocytopenic patients with chronic liver disease. These studies were of limited sample sizes. We conducted a meta-analysis to determine if TPO agonists reduce the need of platelet transfusions before procedures in chronic liver disease patients.
Methods:
We performed a computerized search of Medline, Cochrane and Google Scholar databases through March 2019 for studies evaluating the efficacy of thrombopoietin (TPO) agonists versus placebo in the treatment of thrombocytopenia of chronic liver disease patients undergoing procedures. We screened 295 studies and only 5 of them met our inclusion and exclusion criteria. Inclusion criteria were studies with adults >18 years old, English literature, randomized controlled trials utilizing a TPO agonists in chronic liver disease patients. Exclusion criteria were studies with patients <18 years old, improper study design (e.g. abstract, commentary, editorials) and literature without available data.
The primary study outcomes were proportion of patients responding to TPO agonists in comparison to placebo (an increase of 20000 of platelet count /ul and a value of more than 50000 count/ul). Our secondary outcomes were evaluating the proportion of patients not requiring platelet transfusion and evaluating the percentage of patients who developed a portal venous thrombosis (PVT) on study. Statistical analyses were calculated using Cumulative Meta-Analysis software (version 3.0)
Results:
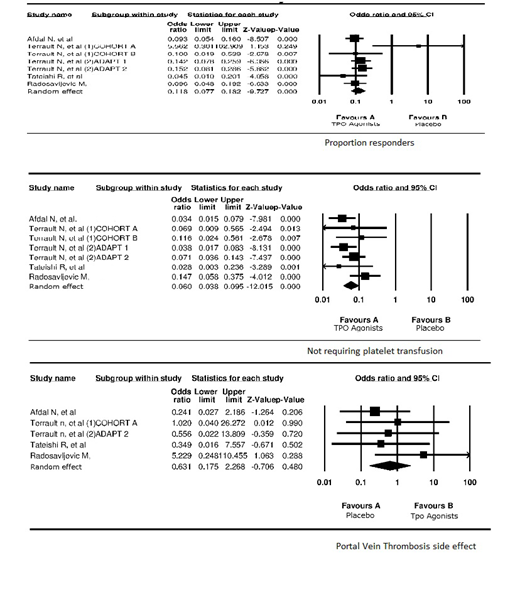
The final analysis included 5 studies with a total of 1098 patients. Please see Image 1 for Individual Trial data. The proportion of responders for TPO agonists odds ratio was 0.060 (0.038-0.095) with P value <0.0001. The proportion of patients not requiring transfusion on TPO agonist odds ratio was 0.118 (0.077-0.182) with P value <0.0001. The portal vein thrombosis odds ratio while on TPO agonist was 0.631 (0.175-2.268) with P value of 0.480.
All 5 trials demonstrated that TPO agonists compared to placebo significantly increased the platelet count and reduced the need of platelet transfusion pre-procedural with a P-value of <0.0001. The risk of developing PVT in patients receiving TPO agonists was not significantly increased when compared to those receiving placebo.
Conclusion:
Our analysis shows that TPO-agonists provide significant benefit compared to placebo in regard to increasing platelet count and reducing the need for platelet transfusions. The risk of developing PVT in patients receiving TPO agonists was not significantly increased when compared to those receiving placebo. More trials are needed to validate the comparison for PVT outcome.
Jaglal:NOVARTIS: Consultancy.

