

BACKGROUND: Severe thalassemia is common in Southeast Asia (SEA) and can lead to transfusion dependent anemia, growth retardation, and perinatal death. Prevention and control of thalassemia can be approached either preconceptionally (through carrier screening, reproductive planning, or preimplantation diagnosis) or antenatally (through prenatal screening and diagnosis and termination of pregnancy). Thailand's national thalassemia program focuses on antenatal interventions, provided free to citizens. However, there is a growing population of migrant workers from neighboring countries who face barriers to healthcare and likely have varied beliefs towards pregnancy termination. We conducted a mixed-methods study using survey, interview, and focus group data to identify key barriers to and optimal strategies for thalassemia screening in migrant communities in Thailand.
METHODS: Myanmar and Cambodian migrant workers and agents, Thai healthcare providers, and Thai adults (aged 18-49 years) at Laem Chabang Hospital (Chonburi, Thailand) participated in a knowledge, attitudes, and practices (KAP) survey, interviews, and focus groups. All sessions were conducted in Thai or English, audio recorded, transcribed and translated into English, and analyzed thematically using MAXQDA. Codes were developed iteratively and used to answer key explanatory questions arising from the KAP survey. Ethical approval for the study was obtained from Mahidol and Duke Universities.
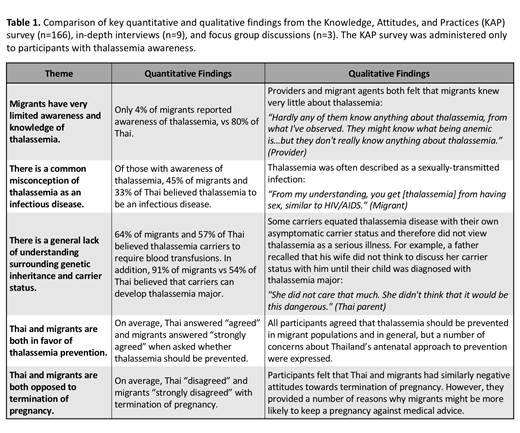
RESULTS: Both quantitative and qualitative data showed dramatically lower thalassemia awareness in migrants vs Thai (Table 1). Furthermore, providers perceived migrants to be disinterested in thalassemia screening, though migrant narratives illustrated significant language barriers, economic barriers, lack of health literacy, and competing social stressors - all of which may contribute to perceived indifference towards thalassemia screening. Both Thai and migrants had misconceptions about thalassemia, believing it to be contagious and sexually transmitted, or equating thalassemia carrier status with disease and vice versa (Table 1). These misconceptions may contribute to the stigmatization and isolation of individuals with thalassemia and disincentivize carrier screening for fear of discrimination.
Participants supported thalassemia prevention and identified antenatal care (ANC) as the main access point for thalassemia education, screening, and prevention. However, they described key limitations of this antenatal approach, including the inability to offer termination in pregnancies presenting late to ANC; couples' hesitation to terminate; cost of prenatal testing (for migrants); and reliance on male partners to present for prenatal testing. In addition, migrants expressed more negative attitudes towards termination of pregnancy on the survey (Table 1). Participants associated this attitude with the perception that migrants were more religious, less educated, less knowledgeable about genetic disease risk, and more eager to have children.
Participants proposed a number of solutions, including targeted education, delivered in migrants' native languages through ANC or public media, and universal carrier screening as a more acceptable approach to thalassemia prevention and control in migrant communities. Recommended settings for screening include schools or universities, hospitals, and workplaces. Migrants also reported relying heavily on employers for access to healthcare. Therefore, employer engagement in thalassemia education and screening efforts is critical, though employment discrimination remains a concern.
CONCLUSION: This study provides insight from a variety of stakeholders into potential barriers and strategies for thalassemia screening in SEA migrant populations. Findings highlight a profound lack of thalassemia awareness among migrants leading to apparent disinterest in thalassemia screening, misconceptions and stigma surrounding thalassemia, and negative attitudes towards termination of pregnancy. Promotion of public education and carrier screening is an optimal strategy for migrant populations in Thailand. Furthermore, this approach can be adopted regionally and cooperatively by member states of the Association of SEA Nations (ASEAN) to better address the shared public health problem of thalassemia.
Telen:Pfizer: Other: Member of a clinical trial steering committee; Novartis: Other: Member of a safety monitoring committee; Forma Therapeutics: Research Funding.

