

Introduction: Deep venous thrombosis (DVT) is a common disease and post-thrombotic syndrome (PTS) is a complication present in about 20-50% of patients after the thrombotic episode (Kahn, 2016 - Hematology Am Soc Hematol Educ Program). The presence of residual venous thrombosis (RVT) can contribute to DVT recurrence and its role in SPT is controversial (Pradoni et al., 2009 - Annals of Internal Medicine; Cosmi et al., 2010 - Eur J Vasc Endovasc Surg). Fibrinolysis is the mechanism responsible for blood clot dissolution and decreased plasma fibrinolytic potential (DPFP), leads to an increased risk of DVT and appears to be associated with PTS, but not with recurrence(Lisman, 2017 - Semin Thromb Hemost; Meltzer et al., 2008 - PLoS Med). Furthermore, hypercoagulability and hypofibrinolysis synergistically enhance the risk of a first venous event, driven probably by elevated plasma levels of TAFI and PAI-1(Bombardier et al., 2012 - Thromb Res; Lisman, 2017 - Semin Thromb Hemost). Relationship between fibrinolysis and DVT has been focused on plasma levels of proteins or protease-inhibitor complexes, and not on plasma fibrinolytic potential (PFP). CloFAL is a turbidimetric assay that calculates the coagulation index (CI) and fibrinolytic index (FI), and allows the evaluation of global fibrinolysis based on clot lysis, with good analytical sensitivity for hypercoagulability and hypofibrinolysis. Preliminary studies of our group demonstrated decreased median fibrinolytic index in patients with lower limb DVT when compared to controls (98% vs 146%, p = 0.003). With the objective to increase scientific knowledge, we evaluated PFP in DVT patients and its association with PTS, RVT, and PAI-1 levels.
Methods: PFP was determined by CloFAL assay and PAI-1 by ELISA method. The reference values of CI and FI were calculated using the median values obtained in plasma samples of 20 healthy subjects, along with the percentiles 25th and 75th (for CI, median was 104%, interquartile range (IQR) = 70-140%; for F, median = 97%; IQR = 80-180%). PTS and RVT were evaluated by Villalta scale and doppler ultrasound (US), respectively. Outpatients with DVT of lower limbs up to two years after the acute episode attended at Hemostasis Clinic of Hemocentro (University of Campinas - UNICAMP, SP Brazil) from 2014 to 2019 were included. Healthy controls were workers from Hemocentro. Exclusion criteria were cancer, anticoagulation, renal or hepatic disease, and infection. Continuous variables among groups were compared with Mann-Whitney test. A multiple regression analysis was performed by to evaluate the effect of age, sex, type of thrombosis (spontaneous or provoked), PAI-1, RVT, time between DVT and blood collection and CI on the observed values of FI.
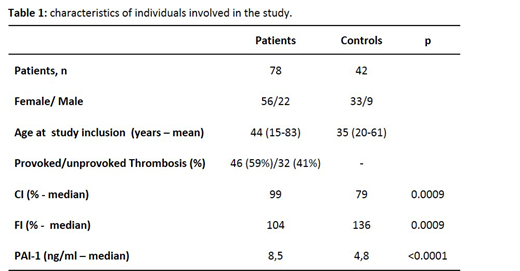
Results: Seventy-eight patients and 42 controls were included. The samples were collected 16 months (range = 1-27) after acute DVT. Forty-three (55%) patients presented PTS and 41 (71%) showed RVT on US. Our results corroborate our previous study, as patients demonstrated a significant increase of CI (p = 0.0009) and decrease of FI (p = 0.0009) (Table 1). However, when patients were analyzed according to the presence of SPT or RVT, no difference was observed. Median PAI-1 levels corrected by BMI were higher in patients compared to controls (8.5 vs 4.8, p< 0.0001). No difference was observed in PAI-1 levels when we compared patients according to SPT and RVT status. When multiple variables were analyzed with a multiple regression analysis, only CI statistically significantly predicted FI (R2= 0.278; p=0.003).
Conclusions: Patients with DVT, even in the chronic phase, presented hypofibrinolysis, when compared to controls. We initially found higher PAI-1 levels in patients when compared to controls but with a multivariate analysis, CI was the only variable that predicted FI. Therefore, other factors not included in this study may contribute to the lower FI values observed in our cohort. The presence of RVT or PTS did not induce modifications of global fibrinolysis.
No relevant conflicts of interest to declare.

