


Objectives
Increasing the intensity of chemotherapy can improve long-term survival in young patients with acute myeloid leukemia, but the number of appropriate courses is still worth exploring. We prospectively used MRC-AML 15 protocol as backbone to designed the C-HUANAN-AML15 protocol, which including 2 courses of inductions and 2 courses of consolidation to treat new diagnosed acute myeloid leukemia children in order to adapt to China's actual situation. The midterm outcome of effectiveness and survival was analyzed in the multicenter of south of China.
Patients and methods
Total of 321 newly diagnosed childhood AML patients from 9 centers of south of China from November 2014 to December 2018 were included in the study. 194 boys and 127 girls, with median age 6 (0.5-14) years old were enrolled. The median follow-up period was 16 (4 to 73) months up to July 2019. Risk stratifications were based on genetic abnormalities and response to induction chemotherapy . One hundred and seven patients (33.3%),146 patients (45.5%),68 patients (21.2%) were classified as low-risk group (LR), intermediate-risk group (IR) and high-risk group (HR) respectively.
The protocol C-HUANAN-AML15 protocol including tandem 2 courses of FLAG-IDA regimen (marked as group A, n=225) , or sequential DAE(3+5+10) and DAE(3+5+8) regimen (marked as group B, n=96) were applied to induction chemotherapy. One course of Homoharringtonine (substitution of Amsacrine in MRC-AML 15 protocol)/ Cytarabine/ Etoposide and one course of Mitoxantrone/ Cytarabine in consolidation chemotherapy were uniform in both groups. 57 patients (39 patients in group A and 18 patients in group B, P=0.752) selected hematopoietic stem cell transplantation (HSCT) after 2-3 courses of chemotherapy. In the 264 patients who only underwent chemotherapy, the LR/IR/HR ratio in the A and B group was 65(34.9%),82(44.1%),39(21.0%) and 34(43.6%),37(47.4%),7(9.0%) respectively (P=0.056).
The similarity of clinical data was analyzed by the chi square test and COX proportional hazard function model. Complete remission (CR) rates, treatment related mortalities (TRM), event-free survival (EFS) and overall survival (OS) were compared by Log-Rank chi square test.
Results
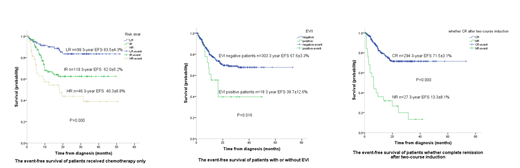
The CR rates in A and B group were 87.6% and 83.3% after 1st course induction regimen, and 92.4% and 89.2% after 2nd course induction regimen, which were not significantly different (P=0.375, 0.337). The 3-year EFS and OS of all patients were 65.8±3.2% and 70.3±3.4% respectively. The 3-year EFS and OS of 264 patients who only received chemotherapy was 65.4±7.4% and 71.7±3.4%. The 3-year EFS of HR, IR and LR in patients who received only chemotherapy were 40.3±8.8%, 62.0±5.2% and 83.5±4.3% respectively (P=0.000). The 3-year OS of HR, IR and LR in patients who received only chemotherapy were 46.9±9.0%, 69.1±5.1% and 86.1±4.0% respectively (P=0.000). The 3-year EFS of A and B group in patients who received only chemotherapy was 70.8±4.0% and 56.7±6.3% (P=0.059); The 3-year OS of A and B group in patients who received only chemotherapy was 78.7±3.6% and 58.6±6.4% (P=0.005). The 3-year EFS and OS of 57 patients who received HSCT was 60.2±8.9% and 65.4±7.4%(P=0.477, 0.821). The EFS of IR and HR patients who received HSCT were superior than that of who received only chemotherapy, but they were not significantly different (78.6±8.6%vs62.4±5.1%, P=0.121; 44.4±12.9%vs38.9±8.8%, P=0.208). Univariate analysis showed that initial white blood cell count (≥50×109/L), RUNX1-RUNX1T1 fusion gene, EVI1 gene positive, FLT3-ITD mutation, no CR after 1st course and 2nd course induction affected 3-year EFS (all P<0.05). Multivariate prognostic analysis with COX proportional hazard function model for EFS showed that EVI1 gene (HR0.397, 95%CI 0.201-0.785, P=0.008) and no CR after 2nd course induction (HR0.319, 95%CI 0.134-0.763, P=0.010) were independent risk factors.
Conclusion
This prospectively clinical study indicated that intensive induction with FLAG-IDA or DAE followed only 2 courses of consolidation chemotherapy was effective in the LR and IR group, and could be utilized as first line treatment in childhood AML. EVI1 gene positive and no CR after 2nd induction course were independent risk factors for EFS. More effective strategies are needed to be explored for HR group patients, EVI1 gene positive patients and those who cannot achieve CR after 2nd course induction.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

