

Introduction:
2-[18F] fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) remains the standard of care for baseline and end of treatment scans for aggressive non-Hodgkin lymphomas (NHLs). However, the role of interim FDG-PET remains not as well defined across aggressive NHLs, especially in the era of high-intensity chemoimmunotherapy. Interim FDG-PET (iPET) can serve as an early prognostic tool, and prior studies evaluating the utility of iPET-guided treatment strategies primarily focused on diffuse large B-cell lymphomas (DLBCL) and frontline R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone). Classification criteria systems assessing response also differ between studies with no clear consensus between use of Deauville criteria (DC), International Harmonization Project (IHP), and the ΔSUVmax method.
Methods:
This study evaluates our institutional experience with iPET during treatment with DA-EPOCH ± R (dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin with or without Rituximab) in aggressive NHLs. We retrospectively evaluated 70 patients at Moffitt Cancer Center who started on DA-EPOCH ± R between 1/1/2014 to 12/31/2018 for aggressive NHLs. Response on interim and end-of-treatment (EOT) scans were graded per DC, IHP, and ΔSUVmax methods, and progression free survival (PFS) probability estimates were calculated with chi-square testing and Kaplan Meier method. PFS outcomes were compared between interim negative and positive scans based on each scoring method. Outcomes were also compared between groups based on interim versus EOT positive or negative scans.
Results:
We identified 70 patients with aggressive NHLs who received DA-EPOCH ± R at our institute. The most common diagnoses were DLBCL (61%) followed by Burkitt's lymphoma (10%), primary mediastinal B-cell lymphoma (9%), plasmablastic lymphoma (7%), gray zone lymphoma (6%), primary cutaneous large B-cell lymphoma (1%), primary effusion lymphoma (1%), and other high-grade NHL not otherwise specified (3%). Of the 43 patients with DLBCL, 21/43 (49%) had double hit lymphoma (DHL) while 7/43 (16%) had triple hit lymphoma (THL), and 3/43 (7%) had MYC-rearranged DLBCL while 2/43 (5%) had double expressor DLBCL. Thirty nine out of 70 (56%) were female, and median age at diagnosis was 58.39 years (range 22.99 - 86.86 years). Most patients had stage IV disease (49/70, 70%), and 43/70 (61%) had more than one extranodal site while 45/70 (64%) had IPI score ≥ 3. Forty-six out of 70 (66%) received central nervous system prophylaxis, most with intrathecal chemotherapy (44/70, 63%).
Fifty-five out of 70 (79%) had iPET available while 6/70 (9%) had interim computerized tomography (CT) scans. Fifty-six out of 70 (80%) had EOT PET, and 4/70 (6%) had EOT CT scans. Sustained complete remission occurred in 46/70 (66%) after frontline DA-EPOCH ± R (CR1), and 12/70 (17%) were primary refractory while 5/70 (7%) had relapse after CR1. Four of 70 (6%) died before cycle 3, and 3/70 (4%) did not have long-term follow-up due to transition of care elsewhere. Median follow-up was 15.29 months (range 0.85 - 60.09 months).
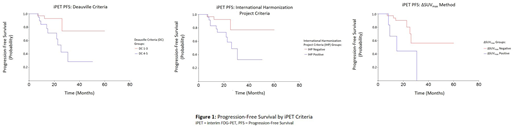
There was significantly better PFS observed if iPET showed DC 1-3 compared to DC 4-5 (Χ2=5.707, p=0.0169), and PFS was better if iPET was negative by IHP criteria (Χ2=4.254, p=0.0392) or ΔSUVmax method (Χ2=6.411, p=0.0113). Comparing iPET to EOT PET, there was significantly better PFS if iPET was negative with EOT PET negative (iPET-/EOT-) compared to iPET positive with EOT negative (iPET+/EOT-), and iPET+/EOT+ and iPET-/EOT+ had worse PFS after iPET-/EOT- and iPET+/EOT- respectively. This pattern in iPET/EOT PFS probability remained consistent when comparing DC (Χ2=30.041, p<0.0001), IHP (Χ2=49.078, p<0.0001), and ΔSUVmax method (Χ2=9.126, p=0.0104). These findings fit clinical expectations with positive EOT scans indicating primary refractory disease. There was no significant difference in PFS when comparing DLBCL versus non-DLBCL (Χ2=3.461, p=0.0628) or DHL/THL versus non-DHL/THL diagnoses (Χ2=2.850, p=0.0914).
Conclusion:
Our findings indicate a prognostic role of iPET during treatment with DA-EPOCH ± R for aggressive NHLs. Significant differences in PFS were seen when graded by DC, IHP, and ΔSUVmax methods used in prior studies and when comparing interim versus EOT response. Larger studies are needed to confirm these findings.
Bello:Celgene: Speakers Bureau. Shah:Novartis: Honoraria; AstraZeneca: Honoraria; Spectrum/Astrotech: Honoraria; Adaptive Biotechnologies: Honoraria; Pharmacyclics: Honoraria; Jazz Pharmaceuticals: Research Funding; Incyte: Research Funding; Kite/Gilead: Honoraria; Celgene/Juno: Honoraria. Sokol:EUSA: Consultancy. Chavez:Janssen Pharmaceuticals, Inc.: Speakers Bureau; Genentech: Speakers Bureau; Kite Pharmaceuticals, Inc.: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees.

