

BACKGROUND:
Diffuse Large B Cell Lymphoma (DLBCL) is the most common hematologic malignancy in adults. Unfortunately, more than one-third of patients will fail first line therapy, highlighting the need for a better understanding of biology of DLBCL and whether biological variables with clinical significance have the same impact across different ethnicities. Two clinically applicable prognostic models in DLBCL are the cell-of-origin (COO) classifier and the MYC/BCL2 expression pattern. The former classifies DLBCL in germinal center B-cell (GCB) and non-GCB subtypes. Patients diagnosed with GCB-like DLBCLs have significantly better outcome than those with non-GCB-like lymphomas. More recently, IHC-based quantification of MYC/BCL2 in DLBCL biopsies was shown to also impart prognostic value, with tumors positive for both markers, named dual-expresser (DE) DLBCL, harboring a particularly poor outcome. Moreover, DLBCL cases are further characterized into "double hit" (DH) or "triple hit" (TH) based on the rearrangements of MYC and BCL2, MYC and BCL6 or MYC, BCL2 and BCL6, which by far exhibit the poorest outcome. The paucity of data comparing the DLBCL biological variables and outcomes among different ethnicities establishes the basis of our analysis at the only NCI-designated cancer center of south Texas within a Hispanic (HI) predominant patient population.
METHODS:
This is an observational study where we identified patients with diagnosis of Lymphoma (Hodgkin and Non-Hodgkin) by International Classification of Diseases (ICD) codes. Only patients with DLBCL were retrospectively analyzed; the patients received care at UT Health San Antonio between 2008-2018. Key variables for each patient included age, gender, race/ethnicity, comorbidities, insurance status, stage, treatment received, characterization by COO, IHC markers, molecular rearrangements, outcome at 3 and 5 years and vitality status in 2018. Continuously distributed outcomes were summarized with the mean and standard deviation and categorical outcomes were summarized with frequencies and percentages. The primary endpoint is to compare whether there are differences between HI and non-Hispanics (NH) with respect to biologic variables and hence their outcomes.
The study was approved by the local Institutional Review Board. The findings will be available to patients, funders and medical community through traditional publishing and social media.
RESULTS:
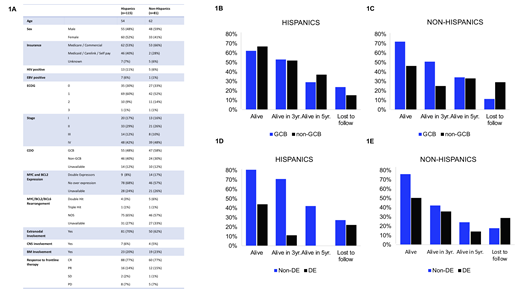
A total of 196 newly diagnosed patients met inclusion criteria, with 115 HI (59%) and 81 NH (41%). HI have a higher percentage (40%) of non-insured, Medicaid or a financial assistance program than NH (28%) . We were able to identify 172 patients with either GCB or non-GCB type. From our HI, 55 (48%) patients were GCB and 46 (40%) were non-GCB while within NH, 47 (58%) patients were GCB and 24 (30%) non-GCB. We gathered IHC data on 147 patients; DE with BCL2/MYC was found in 9 (8%) of HI patients and 14 (17%) of NH patients. There was around the same percentage of unavailable COO and IHC data for both groups, 12% and 25% respectively. Only 11 patients were identified as DH or TH. Among HI, 4 were DH and 1 was TH; while in NH, 5 were DH and 1 was TH (Fig 1A). When looking at survival, as of today 63% of patients are still alive in both groups. Among alive HI, 34 (62%) patients are of GCB origin and 31 (67%) are of non-GCB origin. On the other hand; within the alive NH patients, 34 (72% of GCB positive) are of GCB origin and 11 (46%) are of non-GCB origin (Fig 1B, 1C). Also, DE status apparently had no major difference in survival across ethnicities since 7 (50%) NH remain alive versus 4 (44%) HI (Fig 1D, 1E). Lastly, within HI there are only 2 DH and no TH patients alive, while within NH there are 3 DH patients alive 1 TH patient who is still not 3 years out.
CONCLUSION:
HI have similar and well-balanced molecular characteristics and outcomes compared to NH. As opposed to what we thought, the COO classifier does not seem to predict differences in prognosis in HI as they appear to have equal outcome irrespective of GCB vs non-GCB origin. The prognosis in HI with overexpression of MYC/BCL2 is bad and even worse if DH or TH as historically seen in NH. To our knowledge this is the first retrospective review that includes the largest Hispanic cohort in North America.
Hernandez:ASH MRHAP: Research Funding.

