

Background and rationale
In chronic myeloid leukemia (CML) about half of patients (pts) achieving a deep and stable molecular response (MR) with tyrosine kinase inhibitors (TKIs) may discontinue TKI treatment without disease recurrence. As such, treatment free remission (TFR) has become an ambitious goal of treatment. Given the evidence that deepness and duration of molecular response are necessary but not sufficient requisites for a successful TFR, additional biological criteria to possibly identify more and better CML patients suitable for an efficacious discontinuation are today focus of research in CML. Leukemia stem cells (LSCs) are supposed to be the reservoir of disease. We first showed in a cross-sectional study including 112 pts in TFR for a median of 31 months (mos) that residual circulating CD34+/CD38-/CD26+ CML-specific LSCs were still detectable in the majority of CML pts despite stable and deep molecular response. This evidence suggested that the level of BCR-ABL transcript only may not reflect the actual residual CML LSCs burden and that there could be a "threshold" of LSCs predicting a successful TFR.
Aims
To further study the behavior of residual LSCs during TKI discontinuation we designed a prospective multicentered study (AIRC IG 20133 study) in which we monitored circulating CD26+ LSCs in CML pts from the time of TKI discontinuation until molecular relapse.
Methods
CML pts meeting the current molecular criteria for TKI withdrawal entered this multicenter study. At TKI stop (baseline) and at +1, +2, +3, +6, + 12 mos after discontinuation and at any time if molecular relapse, CML pts were evaluated for peripheral blood number of CD34+/CD38-/CD26+ LSCs by centralized flow-cytometry analysis and for BCR-ABL transcript level by standard (IS) quantitative RT-PCR assay.
Results
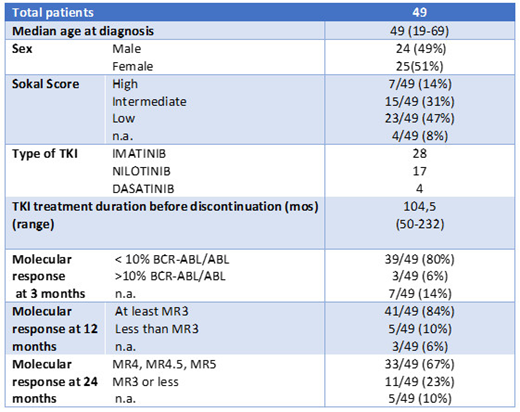
49 consecutive CML pts were enrolled in the study so far. Pts characteristics at diagnosis, type of TKI, disease response and treatment duration before discontinuation are shown in Tab. 1. After a median time of 7 mos since TKI stop (range 1-24), 13/49 (26.5%) pts lost their molecular response and restarted TKI treatment. Median time to relapse after discontinuation was 4 mos (range 2-7). 36/49 (73.4%) pts are still in TFR after a median time of 7.5 mos (range 1-24). If considering a cut-off of 6 mos from discontinuation as the period with higher risk of relapse, 14/36 pts actually in TFR have discontinued treatment for ≤ 6 mos (range 1-6) while 22/36 pts are in TFR for a median of 10 mos (range 7-24). Regarding residual CML LSCs evaluation, at baseline 23/49 (46%) pts had still measurable circulating CD26+LSCs with a median number of 0.0204µ/L (range 0.0077-0.1197), while 26/49 (54%) had no detectable CD26+ LCSs. Considering the small number of molecular relapses no statistical difference in number of residual CD26+ LSCs at time of discontinuation was shown between pts losing vs maintaining TFR (13 pts median CD26+ LSC 0.0237/µ/L, range 0-0.1197 and 36 pts median CD26+ LSCs 0.0204/µ/L, range 0-0.1039, respectively). However, the number of pts with undetectable CD26+ LSCs at baseline was 6/13 (45%) and 20/36 (55%) in the two subgroups, respectively. Considering subsequent time points, the 13 relapsed pts showed a small yet progressive increase of residual CD26+ LSCs number until molecular relapse, while the 36 pts in TFR showed a fluctuation of CD26+ cells number. However, Kendall rank correlation coefficient, Mood test and bi-linear relation model of the whole cohort showed no correlation between BCR-ABL/ABLIS ratio and number of residual CD26+ LSCs either at baseline or at each time points after discontinuation, thus confirming our previous observations.
Conclusions
Yet very preliminary our results showed that CD26+ LSCs are detectable at time of TKI discontinuation and during TFR. Moreover, at least for the observation median time of the study (7.5 mos) the persistence of "fluctuating" values of residual CD26+ LSCs do not hamper the possibility to maintain a stable TFR. Due to the short follow up and the small number of molecular relapsed pts we could not find a threshold of CD26+ LSCs predictive of TFR loss. Our data may suggest other factors then LSCs "burden" to play an active role in controlling disease recurrence. Additional studies evaluating CD26+ LSCs ability to modulate the immune system through a variable expression of immune response inhibitory molecules and through their interactions with effectors cells are ongoing.
Bocchia:Novartis: Honoraria; Incyte: Honoraria; BMS: Honoraria. Pregno:Bristol Myers Squibb: Honoraria; Incyte: Consultancy, Honoraria; Novartis: Honoraria; Pfizer: Honoraria. Abruzzese:Incyte: Consultancy; Novartis: Consultancy; Pfizer: Consultancy; BMS: Consultancy. Crugnola:Novartis: Honoraria; Incyte: Honoraria. Iurlo:Pfizer: Honoraria; BMS: Honoraria; Incyte: Honoraria; Novartis: Honoraria. Galimberti:Roche: Speakers Bureau; Celgene: Speakers Bureau; Novartis: Speakers Bureau. Liberati:Bristol & Mayer: Honoraria; Takeda: Membership on an entity's Board of Directors or advisory committees; Celgene: Honoraria; Servier: Honoraria, Membership on an entity's Board of Directors or advisory committees; Incyte: Consultancy; Amgen: Membership on an entity's Board of Directors or advisory committees; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria.

