

Introduction
Immune dysregulation is a hallmark of CLL, making these patients particularly vulnerable to infectious complications. Patients with CLL are at increased risk of developing varicella zoster virus (VZV) reactivation (shingles) due to their advanced age and immunocompromised status. A new recombinant (non-live) adjuvanted shingles vaccine (SHINGRIX; RZV) has the potential to reduce VZV reactivation, without the risk of giving a live vaccine to immunocompromised individuals. RZV is proven to reduce the risks of herpes zoster and postherpetic neuralgia in healthy adults ≥ 50 years of age, however its efficacy in immunocompromised individuals, including CLL, remains unknown. We report preliminary safety and efficacy of RZV in treated and untreated CLL patients.
Methods
In this phase II open-label study (NCT03702231), patients with CLL who were either treatment naïve or receiving treatment with a Bruton's tyrosine kinase inhibitor (BTK-I) (ibrutinib or acalabrutinib) received 2 doses of RZV via intramuscular injection at 0- and 3-months. Subjects were followed for 6 months and received assessment of serologic response at 3- and 6-months. Based on results of prior published studies, serologic response was defined as a ≥ four-fold rise in VZV anti-glycoprotein E (anti-gE) blood IgG serum titer after completing the RZV vaccine series. Additionally, serologic response was analyzed 3 months following the first vaccine administration to study the kinetics of the humoral vaccine response. All subjects completed an adverse event (AE) diary documenting any local (injection site) or systemic AE that started within 7 days after receiving the first and second vaccine dose. The data reported herein are as of July 12th 2019; updated results will be presented at the meeting.
Results
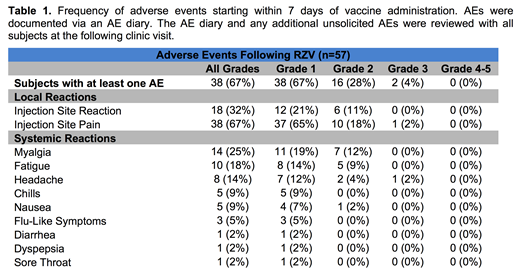
Safety data are available on 57 subjects who received at least one vaccine dose. The most frequent local and systemic AEs were injection site pain (67%), injection site reaction (32%) and generalized myalgias (25%) (Table 1). All adverse reactions were grade 1-2, except for 2 (4%) grade 3 reactions. No serious AEs were reported. All AEs resolved or returned to baseline within 7 days of vaccine administration. Seven subjects have completed the primary endpoint and have had serologic response assessment at 6-months. Serologic responses were observed in 3 (43%) patients. All patients (n = 7) achieved ≥ 2.2-fold rise in VZV anti-gE titers at 6-months. Preliminary analysis of 3-month samples (n = 43) shows early evidence of increasing titers after the first dose of RZV.
Conclusions
RZV administration appears to be safe in CLL patients that are treatment naïve or receiving treatment with a BTK-I. Compared to previously reported toxicities in the healthy population, no increase in frequency or severity of AEs were observed. Preliminary data suggests that RZV induces humoral immune responses in patients with CLL.
Wiestner:Pharmayclics: Research Funding; Acerta: Research Funding; Merck: Research Funding; Nurix: Research Funding.

