

Introduction: Patients with acute myeloid leukemia (AML) may receive more appropriate care when treated regionally instead of locally, but studies have not adequately accounted for baseline differences between regional and local cohorts. In 2015, Kaiser Permanente Northern California, an integrated healthcare delivery system, started to shift AML induction from local (N=21) to regional (N=3) centers. We assessed the association of regionalization with the frequency of use of induction therapy and bone marrow transplantation, and with 60-day mortality.
Methods: Information for all adult health plan members with ≥1 year of enrollment before receiving a diagnosis of AML during 2013-17 was obtained from the electronic health record. Multivariable methods were used to compare risk of induction, bone marrow transplantation, and death before and after 2015 (i.e., 2013-14 and 2016-17) after adjustment for baseline characteristics.
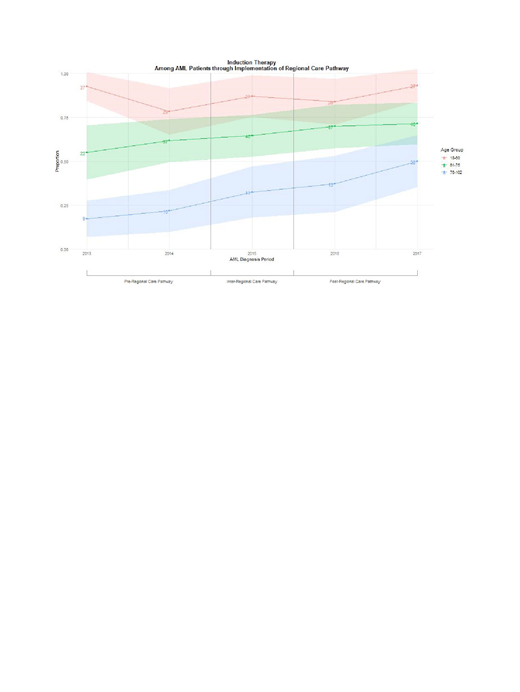
Results: Of 662 patients, 38% were ≥75 years, 30% had an Elixhauser comorbidity index ≥5, and 10% died within the week following diagnosis. Among non-APL patients, we observed increased use of induction therapy (65% vs 49%, p=0.0003) and bone marrow transplantation (23% vs 13%, p=0.007) after 2015, while the 60-day mortality rate did not change (before 2015, 94 of 278 [32.7%]; after 2015, 82 of 249 [32.9%]; p=0.83).
Conclusion: In this community-based population that includes advanced elderly patients with substantial comorbidity, regionalization was associated with increased use of induction therapy and bone marrow transplantation but no increase in the risk of 60-day mortality. Older patients can benefit from AML induction therapy at specialized centers.
No relevant conflicts of interest to declare.

