

Introduction:
One of the critical characteristics of sickle-cell disease (SCD) is the increased rigidity of the red blood cell (RBC) membrane. This decreased flexibility of hemoglobin S (HbS)-rich RBCs contributes to reduced lifespan of the cell and is known to be a primary cause of vaso-occlusion, leading to painful crisis episodes and other complications in SCD. Although often overlooked as a factor in disease severity, increased RBC rigidity has been recently shown to reduce the vascular wall adhesion of white blood cells (WBCs) drastically - hinting at a larger role for RBC rigidity in patient well-being beyond instigating vasocclusion. The rigidity and composition of RBCs in SCD patients varies highly, i.e., there can be a large fraction of HbS cells with moderate stiffness or a small fraction of extremely rigid HbS cells. Ektacytometry is a primary technique used for measuring RBC deformability in SCD via laser diffraction viscometry, but is limited in that it renders an average measurement of deformability for the entire RBC population, i.e., across both stiff and healthy RBCs. This average measurement of deformability may underestimate the rigidity of HbS-rich (%S fraction) or sickle RBC population in the blood. Here, we present an approach to estimate rigidity of HbS cells in SCD via a method that implements artificially rigidified RBCs mixed into whole blood at different ratios.
Methods:
We develop an approach to estimate rigidity of HbS cells in SCD via a method that implements artificially rigidified RBCs. RBCs from healthy (non-SCD) are incubated in solutions with varying concentrations of tert-butyl hydroperoxide to stiffen the cell membrane. These artificially rigidified RBCs are then mixed into whole blood at different ratios/fractions. Four parent concentrations of TBHP are chosen as base RBC rigidities: 1.0, 0.9, 0.75, and 0.5 mM TBHP. After adequate washing, stiffened RBCs are mixed with healthy RBCs in whole blood in increments of 10% rigid RBC fractions up to a total of 100% while holding the hematocrit constant at ~40%. All samples are then measured independently using a LoRRca MaxSis Ektacytometer (Mechatronics Instruments BV, Zwaag, The Netherlands). We then parameterize these ektacytometry deformability measurements to develop a numerical model that predicts the bulk rigidity of the rigid RBC population in SCD blood samples. We measured the EI for fifteen different SCD patient blood samples, details including patient SCD genotype, age, gender, current medical intervention/therapies, %S fraction, and measured maximum bulk EI.
Results:
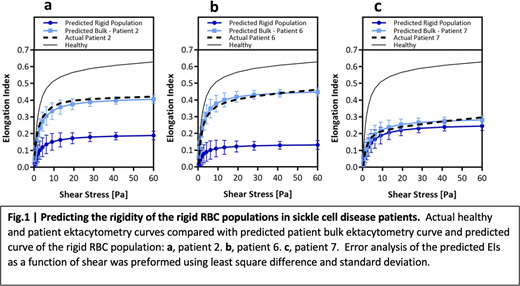
With the predicted maximum EI of the rigid RBC population in patient blood samples, we plotted deformability curves using techniques described by Baskurt et al. We utilized a simplified Skreestra-Bronkhorst model for plotting predicted deformability curves implementing critical parameters such as maximum EI, shear where half the maximum EI is achieved, and the range of shear stress in the standard ektacytometry deformability measurement. The predicted bulk SCD whole blood deformability curves are overlaid with the healthy blood curve, experimental bulk SCD whole blood standard measurement, and with the predicted curve of the sickle RBC population for patients 2, 6, and 7 in Figure 1a, 1b, and 1c. These plots show that the precision of the parameterized deformability curves compared to a standard healthy curve and actual measurement of the patient sample. Specifically, in Figure 1a and 1b shows there is large differences in the elongation curve of the sickle population in comparison to the bulk measurements, yielding a maximum EIs that are ~2 times smaller than the bulk measurement. Conversely, in Figure 1c we see there is not much difference in the elongation curve of the sickle population compared to the actual raw standard measurement.
Conclusions: Overall, this work presents an innovative method for a more thorough examination of ektacytometry deformability measurements of SCD patients. An understanding of bulk stiffness of the HbS population is crucial as it would allow for more accurate characterization of the impact of RBC rigidity on SCD patient crisis and general wellbeing. More detailed information on the rigidity of the HbS RBC population in SCD has the potential to be utilized to understand phenomena in hemodynamics and connection between RBC rigidity and occurrences of painful crisis in SCD patients.
No relevant conflicts of interest to declare.

