

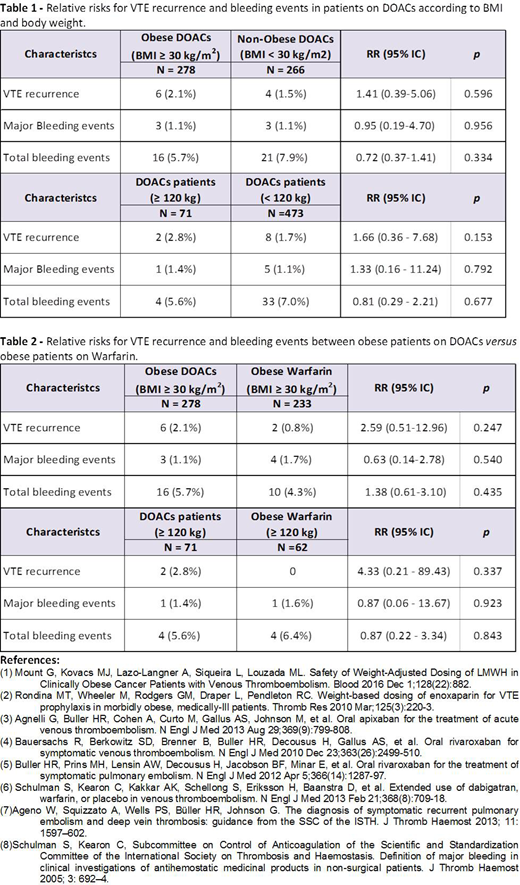
Background: Obesity is a well-known risk factor for venous thromboembolism (VTE), however, obese patients are under-represented in clinical trials (1;2). Four direct oral anticoagulants (DOACs) have been approved for the treatment of acute VTE (3-6), including the direct Factor Xa inhibitors rivaroxaban, apixaban and edoxaban and the direct thrombin inhibitor, dabigatran. Given the lack of data in this population, it is unclear if DOACs can be used safely. Objectives: To evaluate the efficacy and safety of DOACs for the treatment of VTE in obese patients. Methods: We conducted a retrospective, single-centre cohort study in London (Canada) to compare the efficacy and safety of DOACs for the treatment of acute VTE in obese patients. We screened electronic and hard copy charts of adult patients referred to our thrombosis clinic for treatment of an objectively confirmed acute VTE between January 2012 and December 2017. Patients treated with DOACs or Warfarin were selected and followed from diagnosis of the index event until cessation of anticoagulation or up to 1 year. Our study population was analyzed by BMI (BMI ≥ 30 kg/m2versus < 30 kg/m2) and body weight (≥120 kg vs. <120 kg). Patients were excluded if they were on anticoagulation therapy for conditions other than VTE (e.g; atrial fibrillation), cancer-associated thrombosis, or missing data. The primary outcome measure was VTE recurrence during the anticoagulation treatment period and was defined according to the ISTH criteria (7). Our secondary outcome was the occurrence of bleeding events A bleeding event is defined as: a) Major Bleeding: bleed resulting in a hemoglobin drop of > 20 g/L, clinically overt and requiring more than 2 units of packed red blood cells, a hemorrhage requiring permanent cessation of anticoagulation and any retroperitoneal or intracranial hemorrhage; b) Minor Bleeding: bleed with no or little clinical significance, associated with no cost and does not require medical evaluation; and c) clinically significant non-major bleeding: does not fulfill criteria for major or minor bleeding but requires patients to be seek medical attention and/or minor procedures (8). Groups were compared using Chi-square or Fisher's exact test for categorical variables, as appropriate. The significance level was set at 0.05. Risk ratios (RR) and 95% confidence intervals (95% CI) for VTE recurrence and bleeding among DOAC groups and patients treated with Warfarin were analyzed by logistic regression. All statistical analyses were conducted using IBM SPSS Statistics version 25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.). Results: Of 1143 potentially eligible patients, 777 fulfilled our inclusion criteria: 278 (35.8%) obese patients treated with DOACs, 266 (34.2%) non-obese patients on DOACS and 233 (30%) obese patients on Warfarin. Of the patients on DOACs, 80% (n= 436) were on rivaroxaban, while the remaining 20% were either on apixaban or edoxaban (n= 108). Among patients on DOACs VTE recurrence was observed in 2.1% (N=6) of patients with BMI ≥ 30 kg/m2 and 2.8% (N=2) of patients with 120 kg or more, with no differences in the risk of VTE recurrence (Table 1). The proportion of major bleeding events for patients on DOACs was 1.1% (N=3) for patients with BMI ≥ 30 kg/m2 and 1.4% (N=1) for patients with 120kg or more. There were no significant differences with respect to major and total bleeding risk (Table1). When comparing obese patients on DOACs vs Warfarin we did not find differences in the risk of VTE recurrence among patients with a BMI ≥ 30 kg/m2 [RR 2.59 95% IC (0.51-12.96), p= 0. 247] or body weight ≥120 kg [RR 4.33 95% IC (0.21-89.43), p= 0. 337] (Table 2). Among obese patients those treated with DOACs had a similar proportion and risk of total bleeding and major bleeding events compared to those on warfarin (Table 2). Conclusions: Our retrospective study suggests that DOACs at standard doses appear to have similar efficacy and safety in obese patients as defined herein. However, since most of our patients were treated with rivaroxaban, information on other agents is inconclusive. Information on patients with extreme body weight was limited.
Louzada:Bayer: Honoraria; Janssen: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Celgene: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria.

