

INTRODUCTION: Splenic marginal zone lymphoma (SMZL) is a rare and indolent form of NHL with no standard treatment due to scarcity of clinical trials. Watch and wait approach, single agent rituximab or with chemotherapy and splenectomy are valid treatment approaches. No population-based studies examining the impact of chemotherapy and splenectomy on survival of SMZL patients are available. Thus, we decided to compare survival outcomes by clinical factors in SMZL patients deposited in the SEER database, emphasizing in the role of splenectomy on survival outcomes.
METHODS: Retrospective analysis of SMZL cases in the SEER database from 1997 to 2016.SEER collects cancer incidence and survival data from population-based cancer registries covering 34% of the U.S. population. PATIENTS: SEER database was queried for SMZL patients at all ages from 1997 to 2016. Cases without histologic confirmation or no survival data were excluded. Demographic and clinical variables (age, sex, race, ethnicity, B-symptoms, Ann-Arbor stage, DLBCL transformation, first malignancy, chemotherapy with or without rituximab, splenectomy and radiotherapy) were summarized by descriptive statistics. Logistic regression used to determine variables associated with splenectomy. Overall survival (OS) and Cancer-specific survival (CSS) were the major end-points, estimated by Kaplan-Meier method. Cox regression used to calculate Hazard Ratios.
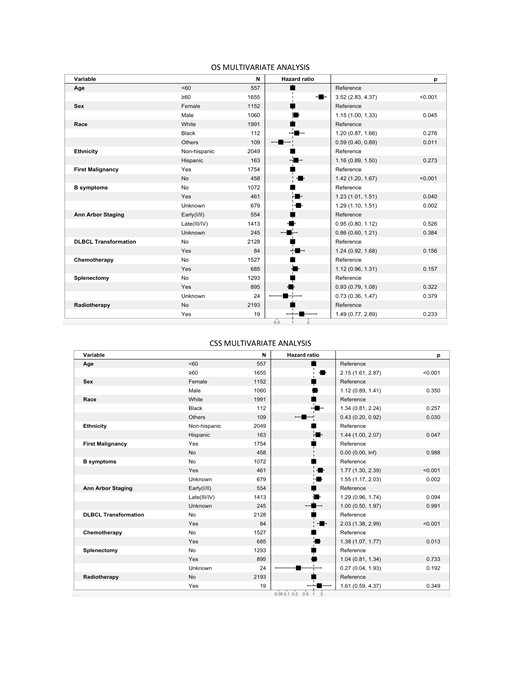
RESULTS: 2212 patients met inclusion criteria, with a median age of 68yo (25-96). Patient characteristics were a follows: males (n=1152, 52.1%); whites (n=1991, 90.0%), blacks (112, 5.1%); Non-Hispanics (n=2049, 92.6%); B-symptoms (n=461, 20.8%); first malignancy (n=1754, 79.3%); Ann-Arbor Stage I (429, 19.4%), Stage IV (n=1351, 61.1%); DLBCL transformation (n=84, 3.8%). Adjusted Odds ratio (aOR) were used to compare splenectomy versus non-splenectomy treated patients: ≥60yo (aOR 0.49;0.40-0.62), males (aOR 0.77;0.64-0.93). Median survival of all the patients was 120 months (95%CI:111-132); On univariate analysis: shorter OS was significantly associated with age ≥60(HR 3.55;2.87-4.38) and non-first malignancy(HR 1.6;1.36-1.88), while shorter CSS was significantly associated with age ≥60(HR 1.76;1.33-2.34), B-symptoms (HR 1.93;1.44-2.60), Stage IV (HR 1.62;1.15-2.28), DLBCL transformation (HR 2.27;1.55-3.33) and treatment with chemotherapy (HR 1.54;1.22-1.94). On multivariate analysis, shorter OS was significantly associated with age ≥60(HR 3.52;2.83-4.37), male sex (HR 1.15;1.00-1.33), B-symptoms (HR 1.23;1.01-1.51) and non-first malignancy (HR 1.42;1.20-1.67). Shorter CSS was significantly associated with age ≥60(HR 2.15;1.61-2.87), Hispanic ethnicity (HR 1.44;1.00-2.07), B-symptoms (HR 1.77;1.30-2.39), DLBCL transformation (HR 2.03;1.38-2.99) and treatment with chemotherapy (HR 1.38;1.07-1.77). Ann Arbor staging and splenectomy were not associated with OS or CSS.
CONCLUSIONS: Older age, Hispanic ethnicity, B-symptoms, DLBCL transformation, and treatment with chemotherapy were associated with poor lymphoma-specific survival. Although, age<60 and female gender were associated higher odds to undergo splenectomy, splenectomy had no impact on the risk of lymphoma-related death or OS. This retrospective study demonstrates that chemotherapy treatment (excluding rituximab) was associated with inferior outcomes in SMZL, while advanced Ann-Arbor stage was not associated with shorter survival as is observed in other indolent lymphomas that commonly present at advanced stage.
Alderuccio:Targeted Oncology: Honoraria; Foundation Medicine: Other: Immediate family member; Agios: Other: Immediate family member; Puma Biotechnology: Other: Immediate family member; OncLive: Consultancy; Inovio Pharmaceuticals: Other: Immediate family member. Lossos:NIH: Research Funding; Seattle Genetics: Membership on an entity's Board of Directors or advisory committees; Janssen Scientific: Membership on an entity's Board of Directors or advisory committees.

