

Background:
The overall incidence of Pneumocystis Pneumonia (PJP) in lymphoma varies according to diagnosis, host factors and treatment rendered.(Carmona, et al. 2011) A meta-analysis suggested that prophylaxis is appropriate when the chance of incurring PJP is 3.5% or greater.(Green, et al. 2007) Accurately characterizing the incidence of PJP is further complicated by a transition in diagnostic methods from direct immunofluorescence assay (DFA) to a DNA-based polymerase chain reaction (PCR) technique.(Caliendo et al., 1998, Wilson JW, et al., 2011) The incidence of PCR-based diagnosis of PJP and the need for anti-Pneumocystis prophylaxis in patients diagnosed with Hodgkin lymphoma receiving chemotherapy requires further investigation.
Methods:
This single center, retrospective, observational study was approved by the Mayo Clinic Institutional Review Board and performed in accordance with the ethical standards of the 1964 Declaration of Helsinki. Consecutive adult patients with a diagnosis of Hodgkin lymphoma receiving chemotherapy between January 2006 and August 2018 were evaluated. Patients with history of bone marrow transplant were excluded. Kaplan-Meier estimation was used to calculate the cumulative incidence of PJP with a 95% confidence interval. Cox proportional hazard models were used to demonstrate the strength of association between the independent variables and PJP rate.
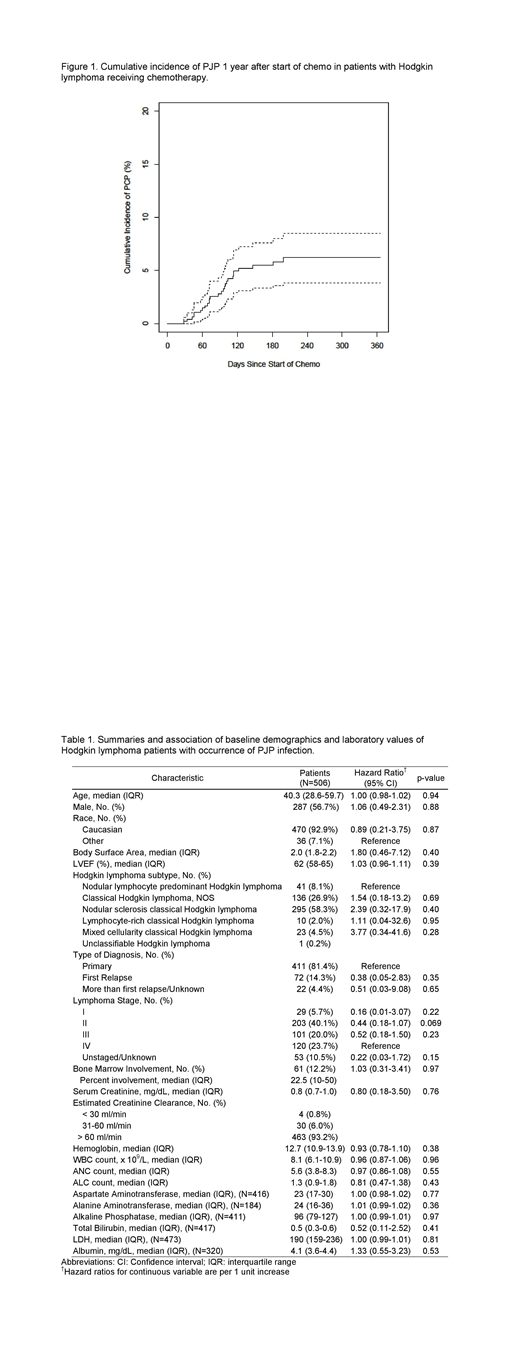
Results: The 506 included patients had a median (IQR) age of 40.3 (28.6, 59.7) years, 287 (56.7%) were male, and 470 (92.9%) were Caucasian. Further baseline demographics and clinical characteristics are described in table 1 with no significant differences between those diagnosed and those free from PJP. Chemotherapy combined with radiation therapy was prescribed for 163 (32.3%) patients while 342 (67.7%) patients received chemotherapy alone. Chemotherapy regimen distribution included 356 patients (70.4%) receiving bleomycin-containing chemotherapy. Median (IQR) total Bleomycin dose was 122 (IQR: 78, 178) Units. Bleomycin-containing combination chemotherapy regimen was not significantly associated with a higher risk for PJP when compared to other combination regimens (HR=1.59, 95% CI 0.55-4.62 p=0.40). Bleomycin-related lung compromise was suspected in 130 (25.7%) patients. Anti-pneumocystis prophylaxis was provided for 97 patients (n=39 a priori, 58 after chemotherapy initiation) and this was not significantly associated with a decreased incidence of PJP (HR=0.51, 95% CI 0.15-1.71, p=0.28). The cumulative incidence of PJP 1 year after start of chemotherapy was 6.2% (95% CI 3.8%-8.5%) and is shown in figure 1. Diagnosis of PJP occurred most commonly during the 2nd (n=8, 30.7%), 3rd (n=8, 30.7%), and 4th (n=7, 26.9%) cycles of chemotherapy. Trimethoprim-sulfamethoxazole was the only agent prescribed as PJP management. There were 10 (38%) patients with PCP that required ICU admission with 9 needing mechanical ventilation, 4 necessitating vasopressor support, and none requiring dialysis. Mortality 30-days from PJP diagnosis was 8% (n=2) with one death attributable to PJP infection.
Conclusion: Cumulative incidence of PJP was 6.2% in patients receiving intensive chemotherapy for Hodgkin lymphoma. As the incidence is above the 3.5% threshold previously described, the clinician should consider the potential value of prophylaxis. Defining the overall utility of universal vs. targeted anti-pneumocystis prophylaxis requires further prospective, randomized investigation.
No relevant conflicts of interest to declare.
Trimethoprim/Sulfamethoxazole, Pentamidine isethionate, and dapsone will be discussed as prevention of Pneumocystis Pneumonia in the HIV-negative population

