

Introduction For patients (pts) with aggressive B-cell lymphoma immunochemotherapy with R-CHOP (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, Prednisolone) represents the standard of care with curative intention. For elderly pts a dose-reduced R-mini-CHOP protocol is feasible. No standard of care exists for frail or very old (>80 yrs) pts not eligible for CHOP-like treatment. Here we present the final results of the prospective DSHNHL-phase-2 trial for old or frail pts receiving Rituximab/Bendamustine (RB) for 1st-line treatment of aggressive B-cell lymphoma. Our goal was to determine feasibility, toxicity of the BR regimen in this pt cohort, and to determine which pts groups might potentially benefit from this reduced-intensity approach.
Methods The open-label, multicenter, prospective, non-randomized phase-II trial "Subcutaneous Rituximab and Intravenous Bendamustine in very Elderly Patients or Elderly Medically Non Fit Patients ("Slow Go") with Aggressive CD20-positive B-cell Lymphoma" (B-R-ENDA, DSHNHL 2010-1, EudraCT 2010-024004-98) included all pts aged ≥81 yrs or 61-80 yrs and elevated CIRS >6, not qualifying for R- CHOP, with histologically confirmed CD20+aggressive lymphoma of any Ann Arbor-stage and IPI score, and ECOG <4 as determined during or after a prephase treatment. During run-in-phase, 20 pts received a prephase treatment of Prednisolone 100mg p.o. d-7 to -1, followed by Rituximab 375mg/m² i.v. on d-3, again followed by 7 cycles of Rituximab 375mg/m² i.v. on d1,q21 and 6 cycles of Bendamustine 90mg/m² i.v. on d1 and 2,q21. After a safety analysis, subsequent pts received prephase treatment with Rituximab 375mg/m² i.v. followed by 7 cycles of subcutaneous (s.c.) Rituximab 1400mg on d1,q21 and bendamustine as above. Primary endpoints were 2-year-progression-free survival (PFS) for efficacy (expected at 30-50% in the >80 yr cohort), and treatment-associated deaths, frequency of grade 3/4 adverse events and SAEs, adherence to the protocol, complete and partial remission rate, rate of primary progression and relapse, and quality of life assessed by geriatric assessment and EORTC-QLQ-C30 for feasibility.
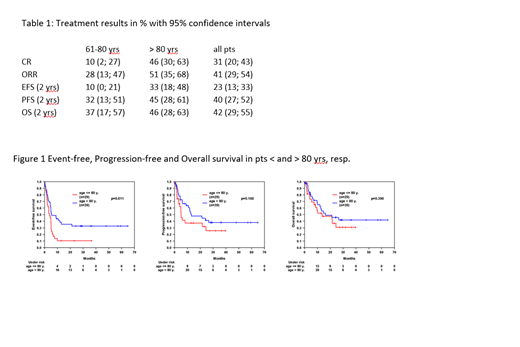
Results: From 2012 to 2016, 68 pts (22 male, 46 female) were recruited in 24 centers into the trial and included into this intent-to-treat analysis (ITT). The median age was 81 yrs with 21% of pts older than 85 yrs. The median CIRS score was 8 and 72% had a CIRS >6. The IPI was >2 in 59% of pts. The patient population was per protocol divided into two subgroups: pts 61 to 80 yrs old and medically non-fit (29 pts) and pts older than 80 yrs (39 pts). For the 61 to 80 yrs old medically non-fit patients median age was 77 yrs (64-80), median CIRS score was 10 (2-22), IPI was > 2 in 76% of pts, 66% of pts had stage 3 or 4 disease, and ECOG was >1 in 52% of pts. For the subgroup of pts > 80 yrs, median age was 84 yrs (81-95), median CIRS score was 7 (1-17), IPI was > 2 in 46% of pts, 51% of pts had stage 3 or 4 disease, and ECOG was >1 in 23% of pts. 49% of pts received the complete treatment as planned (61-80 yrs: 38%; >80 yrs: 56%). Reasons for early termination of treatment were PD in 15% (17%; 13%) and toxicity in 24% (24%; 23%) of pts. 29% 95% Confidence interval 19-42% of pts (38%; 23%) had grade 3-5 infections. Treatment related mortality was 15% (17%; 13%). Overall response rate (ORR) was 41% (28%; 51%) with 31% CR (10%; 46%). Median observation time was 29 months for EFS, PFS and OS. 2-yrs EFS was 23% (10%; 37%), PFS was 40% (32%; 45%), OS was 42% (37%; 46%). In a multivariate analysis adjusted for IPI factors elevated LDH and ECOG >1 constituted the most significant risk factors for poor outcome.
Conclusions: We describe a frail patient cohort with a median CIRS score of 8, with 72% pts with a CIRS >6, considerable comorbidities and a high percentage of high-risk IPI. The primary efficacy endpoint (2 yr PFS > 80 yrs 45%) was met; for R-mini-CHOP, this was reported at 47% (Peyrade et al., Lancet Haemat, 2011). The IPI predicts outcome in the >80 yrs cohort reliably. The RB regimen is active even in very elderly and frail pts up to 90 yrs of age. Therefore, in pts not eligible for full- or reduced dose R-CHOP treatment, it represents a tolerable and efficient alternative, albeit with a limited curative potential preferably in IPI low/intermediate-risk pts. Biomarker, comorbidity and QoL data will be analysed subsequently.
Zettl:Roche: Other: travel grants, Research Funding; Mundipharma: Research Funding. Viardot:Kite/Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Honoraria; F. Hoffmann-La Roche Ltd: Honoraria, Membership on an entity's Board of Directors or advisory committees. Korfel:Mundipharma: Consultancy, Research Funding. Dreyling:Janssen: Consultancy, Other: scientific advisory board, Research Funding, Speakers Bureau; Novartis: Other: scientific advisory board; Gilead: Consultancy, Other: scientific advisory board, Speakers Bureau; Sandoz: Other: scientific advisory board; Acerta: Other: scientific advisory board; Celgene: Consultancy, Other: scientific advisory board, Research Funding, Speakers Bureau; Mundipharma: Consultancy, Research Funding; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: scientific advisory board, Research Funding, Speakers Bureau; Bayer: Consultancy, Other: scientific advisory board, Speakers Bureau. Illmer:Roche: Other: travel support. Schmitz:Novartis: Honoraria; Gilead: Honoraria; Celgene: Equity Ownership; Riemser: Consultancy, Honoraria. Klapper:Roche, Takeda, Amgen, Regeneron: Honoraria, Research Funding. Poeschel:Hexal: Speakers Bureau; Roche: Other: Travel support; Amgen: Other: Travel support; Abbvie: Other: Travel support; Astra Zeneca: Other: Travel support. Truemper:Takeda: Consultancy, Research Funding; Roche: Research Funding; Seattle Genetics, Inc.: Research Funding; Mundipharma: Research Funding; Janssen Oncology: Consultancy; Nordic Nanovector: Consultancy.

