

Introduction
The majority of prognostic indexes in CMML include information extracted from bone marrow (BM) evaluation. The blast count in BM in CMML includes the blast and promonocyte percentage. In the extent of our knowledge there are no data evaluating whether both cells have an equivalent prognostic weight for predicting survival. Recent data indicate that an accurate diagnosis of CMML could be established by assessing the monocyte population distribution by flow cytometry and by evaluating its molecular profile by targeted next-generation sequencing in PB.
Our aim was to analyze which variables from our series had an independent prognostic value in order to assess if their addition to the most common prognostic scores for CMML, CPSS and Mayo prognostic model (Mayo), contributed to increase their predictive capacity; or if they allowed us to create a new one.
Methods
One hundred and fifty patients diagnosed with CMML from 1975 to 2019 from a single institution were evaluated. All patients met 2017 WHO criteria. Complete information was available for the following: BM blast percentage, BM promonocyte percentage, PB blast percentage, circulating immature myeloid cells (IMC), presence of Auer rods and complete blood count. The median overall survival (OS) was 35 months (CI 95%: 30-40). We performed univariate and multivariate survival analyses to establish the prognostic weight of each one. Both C-index and Somers'D (Dxy) were used to compare the prognostic accuracy of the different models.
Results
Patients characteristics are depicted in Table 1.
The prognostic impact of the following items was reviewed: BM blasts; BM promonocytes; the sum of BM blasts and promonocytes; proliferative CMML (CMML-P); monocyte count ≥ 5 x 109/L; transfusional dependency; Hb < 100 g/L; platelets < 100 x 109/L; IMC; PB blasts; abnormal karyotype; spanish cytogenetic risk classification; sex, and dysmegacaryopoiesis, dysgranylopoiesis and dyserythropoiesis according to WHO criteria.
In the univariate analysis for the OS only the following demonstrated an adverse impact: sex (women 50.7m vs men 33.4m, P=0.023), PB blasts (39m vs 11m, P<0.001), BM blasts ≥ 10% (35.7m vs 21.6m, P=0.033), Hb < 100 g/L (40.9m vs 21.7m, P=0.001), platelets < 100 x 109/L (40.9m vs 31.6m, P=0.004), abnormal karyotype (39.4m vs 31.6, P=0.01), spanish cytogenetic risk classification (37.5m vs 5.4m vs 9.2m, P=0.001), monocyte count ≥ 5 x 109/L (31.6m vs 35.7m, P=0.02), and leucocyte count ≥ 13 x 109/L (24.1m vs 39.8m, P=0.005). As shown, we did not observed an adverse impact on OS when assessing the percentage of promonocytes as continuous variable or categorized at 5% or 10% cut-offs. Only PB blasts, Hb < 100 g/L and platelets < 100 x 109/L maintained their adverse impact in a multivariate cox regression analysis including all the variables that showed an impact in the univariate analysis. These variables maintained their independent prognostic impact when adjusted for sex and age. The Hazard Ratios (HR) were: 2.9, 1.9, 1.7 for PB blasts, Hb and platelets
The CPSS and Mayo prognostic model accurately stratified the prognosis in our series, having the last one a higher predictive capacity for the OS (C-index: 0.62 vs 0.65; Dxy: 0.24 vs 0.3). The prognostic accuracy of the CPSS improved when the platelets were added (CPSS-P) (C-index 0.63; Dxy: 0.26).
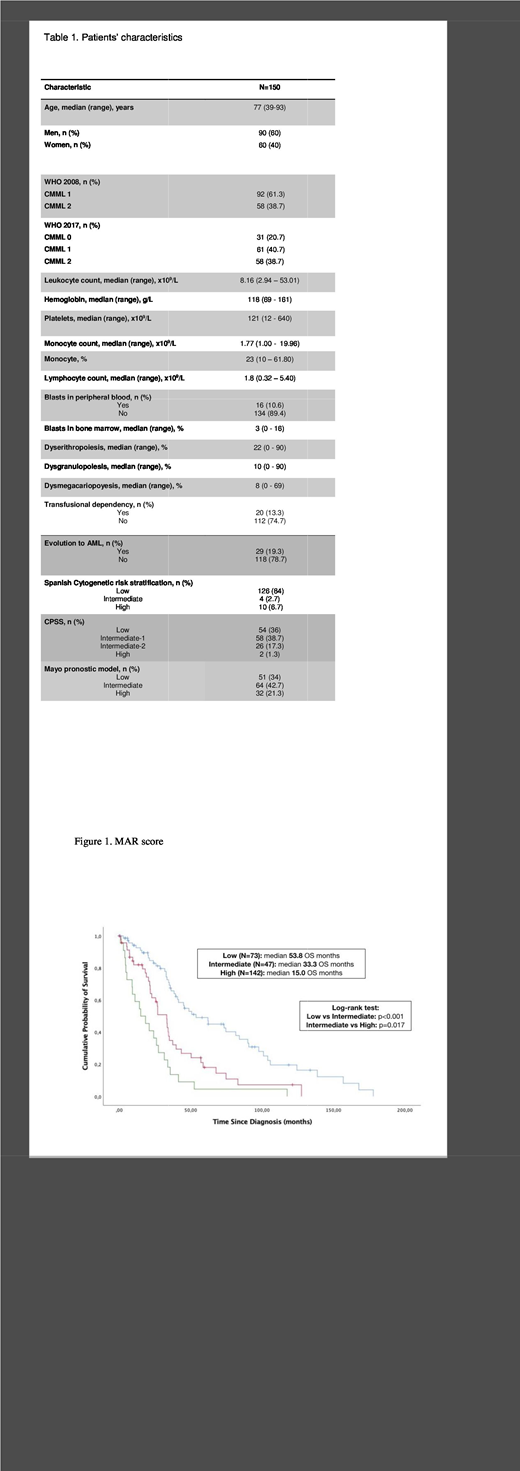
Given the prognostic weight of the three values described, we developed a score based on these: platelets < 100 x 109/L, 0.5 points; Hb < 100g/L, 1 point, and PB blasts, 2 points. The MAR score (Figure 1) segmented the series in three risk categories with significant differences in OS: low (0 points), median OS 54m; intermediate (0.5-1 points), median OS 33m; and high (1.5-3.5 points), median OS 15m. The MAR score showed a better value for C-index (0.66) and Dxy (0.32) than the rest of scores assessed.
Conclusions
The variables with an independent adverse prognostic value for OS in our series were: Hb < 100 g/L, platelets 100 x 109/L and the presence of blasts in PB. The MAR score, a model based on them showed the best predictive capacity for OS in our series.
No relevant conflicts of interest to declare.

