

Some of the recurrently occurring somatic mutations are known to be diagnostic or prognostic in myelodysplastic syndrome (MDS). Targeted gene capture and next-generation sequencing (NGS) has rapidly become routine clinical tools to detect the somatic mutations in patients with MDS. Copy number variants (CNVs) may have additional clinical significance in MDS. Chromosomal microarray analysis is a standard technique for genome-wide CNV detection, but multiple testing strategies require high costs and time. Recent advancements in NGS technologies have developed more cost-effective and rapid methods to allow simultaneous identification of targeted CNVs as well as somatic mutations using the same panel-based NGS data. In this study, we investigated whether the detection of CNVs using the targeted NGS data provided an additional value other than the clinical implications of somatic mutations.
We performed targeted deep sequencing analysis on bone marrow samples obtained from 266 patients with MDS using an MDS panel targeting 28 well-known MDS-related genes (NRAS, DNMT3A, SF3B1, IDH1, TET2, NPM1, LAMB4, EZH2, JAK2, CBL, ETV6, KRAS, FLT3, IDH2, PRPF8, TP53, NF1, SRSF2, SETBP1, DNMT1, ASXL1, RUNX1, U2AF1, ZRSR2, ATRX, STAG2, MMP8, and ARID2). Sequencing libraries were generated using the AmpliSeq Library Kit 2.0 (Life Technologies, Carlsbad, CA) and the MDS panel was then sequenced using the Ion Torrent Proton system (Life Technologies) according to the manufacturer's instructions. The multiscale reference module and Rank Segmentation statistical algorithm in NEXUS software v9.0 (Biodiscovery) were used to define the CNVs for each sample. Overall survival (OS) and acute myeloid leukemia (AML)-free survival (AFS) were estimated from the date of MDS diagnosis to death or AML progression using the Kaplan-Meier method, and the differences in survival were compared using the log-rank test (for univariate analysis) and the Cox proportional hazards model (for multivariate analysis).
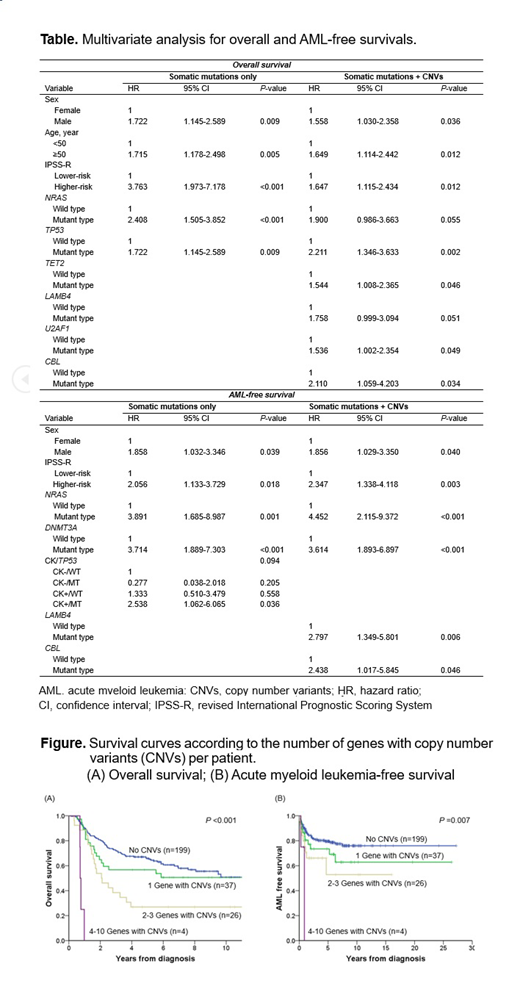
Overall, 215 patients (80.8%) carried at least one somatic mutations, and 67 (25.2%) had one or more CNVs. The number of mutated genes per patient ranged from 0 to 6, and the number of genes with CNVs per patient ranged from 0 to 10. Of 51 patients who did not have somatic mutations, 12 (23.5%) had the targeted CNVs. The mutated genes in more than 10% of patients were 8: U2AF1 (21.8%), TET2 (17.7%), ASXL1 (13.5%), TP53 (13.2%), SETBP1 (12.8%), NF1 (10.9%), SF3B1 (10.5%), and RUNX1 (10.5%). The genes with CNVs detected in 10 or more patients were 5: EZH2 (loss in 7q, 6.8%), KRAS (gain and loss in 12p, 5.3%), ASXL1 (gain and loss in 20q, 4.5%), LAMB4 (loss in 7q, 3.8%), and RUNX1 (gain and loss in 21q, 3.8%). Interestingly, all five patients with TP53 deletion exhibited TP53 mutation as well, suggesting a bi-allelic alteration (mutation + copy loss). The higher number of genes with CNVs per patient were significantly associated with inferior OS (P <0.001) and AFS (P=0.007) (Figure). Considering clinical variables and somatic mutations only, multivariate analysis demonstrated that sex, IPSS-R, NRAS mutation, and TP53 mutation were independent prognostic factors for OS, and sex, IPSS-R, NRAS mutation, DNMT3A mutation, and complex karyotype/TP53 mutation were independent prognostic factors for AFS. When we consider clinical variables and both somatic mutations and CNVs, genetic alterations in TET2, LAMB4, U2AF1, and CBL showed additional significant impact on OS or AFS (Table).
Our study suggests that simultaneous detection of targeted CNVs as well as somatic mutations using the same panel-based NGS data add clinically useful information on the prognosis of MDS patients.
No relevant conflicts of interest to declare.

