

Introduction
In chronic lymphocytic leukemia (CLL), few randomized clinical trials include patients who are older or have significant comorbidity, despite constituting a large proportion of the CLL-population. Therefore, detailed data on the association of specific comorbidities with CLL-prognosis are missing and decisions on treatment and follow-up are poorly informed in comorbid patients. We present data on the association of comorbidity with prognostic factors, treatment patterns and causes of death in patients from the world's largest cohort of unselected CLL-patients.
Methods
All patients diagnosed with CLL in the CLL-registry (2008-2017) or the Danish Cancer Register (1997-2017) were followed through the Civil Registration System from 1 month after CLL-diagnosis until death, emigration or January 2017. Data from Danish nationwide population-based health registers were linked through personal unique identification numbers. Data on comorbidities based on the modified Charlson Comorbidity Index was attained from the Danish National Patient Register, from 20 years prior to the CLL-diagnosis and until 1 month after. Multimorbidity was defined as ≥ 2 comorbidities. Prognostic baseline data such as Binet Stage, IGHV-status, cytogenetics and β2-microglobuline (B2M) level were available through the CLL-registry. Causes of death were ascertained through the National Register of Causes of Death, further sub-categorized as CLL-related (including CLL, all other malignancies and infections) and CLL-unrelated death. Hazard ratios (HR) for mortality were calculated using Cox regression models, adjusting for age, sex, calendar period (5-year intervals) and internally for all other comorbidities. The association between IGHV-status and overall survival (OS) and treatment-free survival (TFS) was assessed by means of Kaplan-Meier and fully adjusted Cox models, stratifying for age and comorbidity-burden.
Results
The study included 8055 patients with a median follow-up time of 4.2 years; 59 % were male and the median age at diagnosis was 71 years. Overall 2816 patients (35%) were comorbid and 965 (12%) multimorbid. At diagnosis 818 (10%) patients had a history of chronic heart failure or myocardial infarction, 672 (8%) cerebrovascular disease, 626 (8%) diabetes (type 1 or 2), 620 (8%) chronic pulmonary disease, 399 (5%) peripheral vascular disease, 307 (4%) peptic ulcer, 264 (3%) connective tissue disease, 172 (2%) psychiatric disease, 148 (2%) renal disease, 87 (1%) dementia and 86 (1%) hepatic disease. Elevated B2M (>4.0 mg/L) was more common in comorbid (20%) and multimorbid (24%) patients compared with non-comorbid (11%), while Binet Stage B/C, unmutated IGHV-status and del(17p) were evenly distributed across the groups (18-20%, 31-33% and 6-8%, respectively).
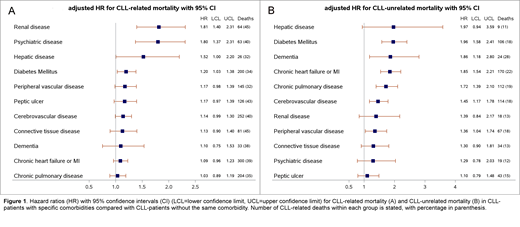
Among comorbid patients, 56% died during follow-up, compared with 42% among non-comorbid patients. For comorbid patients, death was more commonly caused by cardiovascular disease (14% vs 6%) or other causes (14% vs 10%), while hematological malignancy was less common (25% vs 34%) compared with non-comorbid patients. Other malignancies (11% vs 13%), infection (34% vs 35%) and cerebrovascular disease (2% vs 2%) were equally common causes of death in the two groups. All individual comorbidities were associated with increased all-cause mortality. Except for connective tissue disease, dementia and chronic pulmonary disease, all comorbidities were associated with increased CLL-related mortality (Fig 1A) and as for CLL-unrelated mortality, only ulcer disease, psychiatric disease, renal disease and connective tissue were not associated with an increase.
Unmutated IGHV status was associated with inferior TFS for all patients regardless of age and comorbidity burden (range of HRs 1.47-3.70), while IGHV status was associated with inferior OS for non-comorbid patients only (range of HRs 1.43-1.66). Of comorbid patients who died from CLL-related causes, 59% had not received treatment for CLL, compared with 43% among non-comorbid patients.
Conclusions
All individual types of comorbidity were associated with increased all-cause mortality and most also with higher CLL-related mortality. Improved management is warranted for comorbid CLL-patients, who should be prioritized in clinical trials of agents with high tolerability to further inform treatment guidelines and reduce CLL-related mortality for these patients.
Curovic Rotbain:Abbvie: Other: Travel Grant; AstraZeneca: Consultancy, Research Funding; Janssen: Research Funding. Niemann:Novo Nordisk Foundation: Research Funding; AstraZeneca: Consultancy, Other: Travel Grant, Research Funding; Sunesis: Consultancy; Acerta: Consultancy; CSL Behring: Consultancy; Roche: Other: Travel Grant; Janssen: Consultancy, Other: Travel Grant, Research Funding; Abbvie: Consultancy, Other: Travel Grant, Research Funding; Gilead: Other: Travel Grant. Da Cunha-Bang:Janssen: Consultancy; Abbvie: Consultancy, Other: Travel Grant; AstraZeneca: Consultancy; Roche: Other: Travel Grant. Frederiksen:Gilead: Research Funding; Abbvie: Research Funding; Janssen Pharmaceuticals: Research Funding; Novartis: Research Funding; Alexion: Research Funding.

