

Background:
Sickle cell disease (SCD) affects 100,000 adults and children in the United States (USA). Painful, uncomplicated vaso-occlusive episodes (VOE) are the most common complication of SCD and the #1 reason adults with SCD seek medical attention in the ED. The NHLBI guidelines suggest encouraging oral hydration, along with analgesics, during VOE but to give intravenous (IV) fluids only if the patient cannot drink. However, there exists a clinical equipoise regarding the choice of IV fluids to use during the treatment of VOE in the ED, along with the rate or volume given. Despite lack of guidelines or evidence, the use of large IV volumes of crystalloids given over short periods of time (i.e. bolus) in the ED is common practice and we recently showed normal saline (NS) boluses in particular may be associated with inferior pain control and higher admission rates in pediatric patients with VOE (Carden etal., Am J Hem, 2019). Importantly, investigations into the use and impact these different IV fluids, including IV boluses, and how they may impact clinical outcomes among adult patients with SCD and VOE who present to the ED are lacking.
Methods:
We conducted a cross-sectional survey of emergency providers at the 2011 annual American College of Emergency Physicians Scientific Assembly, where ED providers from across the United States attend, regarding IV fluid practices during VOE. We specifically used a validated instrument to assess self-reported practices toward patients with SCD regarding IV fluid use, including volumes and rates, during uncomplicated VOE. Basic demographic information was obtained and providers were specifically asked: "Please indicate which type of fluids and rate of administration you give to patients with acute sickle cell pain who are not hypotensive and not severely hypovolemic". Providers responded never, rarely, frequently or always to each fluid type and rate.
Results:
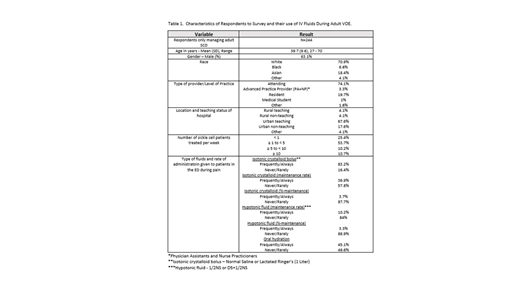
Of 795 respondents to the survey, 722 indicated they took care of patients with SCD, 669 completely responded to the survey, and of those, 244 respondents only took care of adult patients with SCD. Demographic and experience with SCD patients, as well as preferred fluid type and rate of administration is reported in Table 1. IV fluid use during uncomplicated VOE varied among adult providers, but 83% of providers surveyed used IV fluid crystalloid boluses during VOE. Only 45% of providers recommended oral hydration during VOE among adults.
Conclusions:
Among adults ED providers who care for patients with SCD in the USA, wide variations in practice utilizing IV fluids are common. Despite no guidelines, IV fluid boluses are commonly given, as was seen in pediatric ED studies, and oral hydration is less commonly recommended among adult ED providers. Further investigation is needed to determine if these practices have an impact on clinical outcomes among euvolemic adult patients with SCD and VOE who present to the ED.
Carden:GBT: Honoraria; NIH: Research Funding. Tanabe:NIH: Research Funding; AHRQ: Research Funding. Glassberg:ACEP: Research Funding; NHLBI: Research Funding; Pfizer: Research Funding.

