


Aplastic anemia (AA) is an immune-mediated bone marrow failure, resulting in reduced number of hematopoietic stem and progenitor cells and pancytopenia. The presence of paroxysmal nocturnal hemoglobinuria (PNH) clone in AA usually suggests an immunopathogenesis in patients. However, when and how PNH clone emerge in AA is still unclear. Hepatitis associated aplastic anemia (HAAA) is a special variant of AA with a clear disease course and relatively explicit immune pathogenesis, thus serves as a good model to explore the emergence and expansion of PNH clone.
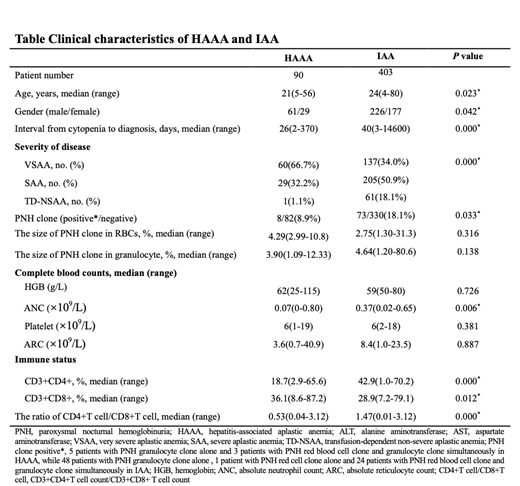
To evaluate the frequency and clonal evolution of PNH clones in AA, we retrospectively analyzed the clinical data of 90 HAAA patients that were consecutively diagnosed between August 2006 and March 2018 in Blood Diseases Hospital, and we included 403 idiopathic AA (IAA) patients as control. PNH clones were detected in 8 HAAA patients (8.9%,8/90) at the time of diagnosis, compared to 18.1% (73/403) in IAA. Eight HAAA patients had PNH clone in granulocytes with a median clone size of 3.90% (1.09-12.33%), and 3 patients had PNH clone in erythrocytes (median 4.29%, range 2.99-10.8%). Only one HAAA patients (1/8, 12.5%) had a PNH clone larger than 10%, while 24 out of 73 IAA patients (32.9%) had larger PNH clones. Taken together, we observed a less frequent PNH clone with smaller clone size in HAAA patients, compared to that in IAAs.
We next attempted to find out factors that associated with PNH clones. We first split patients with HAAA into two groups based on the length of disease history (≥3 mo and < 3mo). There were more patients carried PNH clone in HAAA with longer history (21.4%, 3/14) than patients with shorter history (6.6%, 5/76), in line with higher incidence of PNH clone in IAA patients who had longer disease history. Then we compared the PNH clone incidence between HAAA patients with higher absolute neutrophil counts (ANC, ≥0.2*109/L) and lower ANC (< 0.2*109/L). Interestingly, very few VSAA patients developed PNH clone (5%, 3/60), while 16.7% (5/30) of non-VSAA patients had PNH clone at diagnosis. We monitored the evolution of PNH clones after immunosuppressive therapy, and found increased incidence of PNH clone over time. The overall frequency of PNH clone in HAAA was 20.8% (15/72), which was comparable to that in IAA (27.8%, 112/403). Two thirds of those new PNH clones occurred in non-responders in HAAA.
In conclusion, PNH clones are infrequent in HAAA compared to IAA at the time of diagnosis, but the overall frequency over time are comparable between the two groups of patients. In SAA/VSAA patients who are under the activated abnormal immunity, longer clinical course and relatively adequate residual hematopoietic cells serve as two important extrinsic factors for HSCs with PIGA-mutation to escape from immune attack and to expand.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

