

Introduction: The prevalence of thrombosis in lymphoma patients is reportedly high and ranges from 3 - 10%, and further increased at advanced stages of the disease especially in hgNHL. Inflammation and other vascular factors contribute to the pathogenesis of these thrombotic complications. Biomarkers of hemostatic activation, vascular dysfunction and inflammation are elevated in lymphoma. We have previously reported that thrombin generation biomarkers such as D-Dimer, thrombin anti-thrombin complex (TAT) and prothrombin fragment (F1.2) along with inflammatory biomarkers are increased in cancer patients. Interestingly, despite an increase in thrombin generation markers, thrombin generation potential in these patients is decreased. This study was designed to compare the thrombin generation potential and its relevance to the generation of various biomarkers of hemostatic activation process and inflammatory responses.
Methods: Citrated blood samples from 90 patients with confirmed diagnosis of non-Hodgkin lymphoma (NHL), Hodgkin lymphoma (HL) and Chronic lymphocytic leukemia/Small lymphocytic lymphoma (CLL/SLL) were collected from the Clinic of Hematology Unit, University of Belgrade, Belgrade, Serbia. 50 samples of normal human plasma (NHP) was obtained from George King Biomedical (Overland park, KS). NHP was prepared for referencing purposes. Thrombin generation studies were carried out using a commercially available a kinetic fluorogenic substrate method (calibrated automated thrombogram; CAT). Thrombin generation parameters such as peak thrombin (PT), lag time (LT) and area under the curve (AUC) were compiled. Plasma levels of D-Dimer, CRP, vWF and TNF- α were measured by using commercially available Sandwich ELISA assays. Results were compiled in terms of mean ± SD. Correlation analysis carried out by using Prism, Graphpad.
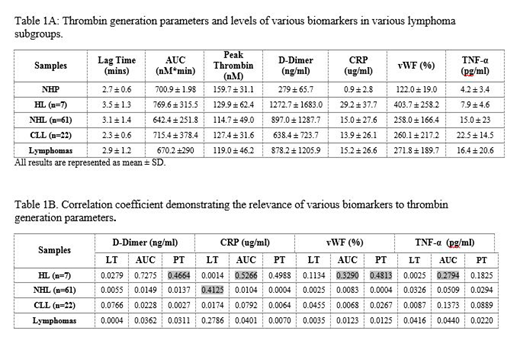
Results: On a cumulative basis, lymphoma patients showed an increase in lag time (2.9 1.17) in comparison to the NHP (2.7). The peak thrombin levels was decreased (119.0 46.2) in the lymphoma patients in comparison to NHP (159.7 31.1). The AUC was decreased (670.2 290.01) in the lymphoma patients in comparison to NHP (700.9 ). When the lymphoma patients were sub grouped, peak thrombin levels were similar in HL (129.9), NHL (114.7) and CLL (127.4) and were decreased compared to NHP (159.7). However the AUC was increased in the HL (769), decreased in NHL (642.4) and was comparable for CLL (715.4) compared to NHP (700.9). Variations in lag time were noted in the three groups. The lymphoma patients also exhibited elevated levels of D-Dimer (878 1205 ng/ml) in comparison to NHP (280 ng/ml), CRP (15.2 26.6 ug/ml) in comparison to NHP (0.9 ug/ml), vWF (271.8 189.7 %) in comparison to NHP (122%) and TNF-α (16.4 20.64 pg/ml) in comparison to NHP (4.2 pg/ml). Interestingly, when the lymphoma group were subdivided into various groups, the D-Dimer level was highest in HL following the order HL>NHL>CLL. CRP and vWF levels were highest in HL and comparable in both NHL and CLL. Wide scatter in TNF-α data was noted with CLL exhibiting highest levels with the ranked order CLL>NHL>HL. The composite data on thrombin generation parameters and biomarkers is shown on the table 1A. In the HL group D-Dimer and CRP correlated well with AUC and PT, in this group vWF also showed a good correlation with PT. In the NHL group, CRP correlated well with LT. In the CLL group none of the biomarkers correlated well with the thrombin generation parameters. On a cumulative basis, D-Dimer, CRP, vWF and TNF-α had no significant relevance to thrombin generation parameters. The composite regression coefficience data is shown on table 1B.
Conclusion: Lymphoma patients represent a heterogenous group in which both the hypercoagulable state and inflammatory responses simultaneously occur as evident by increase in D-Dimer and inflammatory biomarkers. While the overall thrombin generation potential in the plasma of these patients is decreased, thrombin is constantly generated in some of these patient leading to the formation of fibrin. The observed decrease in thrombin generation potential in these patients may be due to the consumption of prothrombin and other coagulation factors. Wide variations among these lymphoma groups are noted. Profiling of thrombin generation and inflammatory biomarkers may be helpful in thrombotic risk stratification of lymphoma patients and their anti-thrombotic management.
No relevant conflicts of interest to declare.

