

Background: Tisagenlecleucel is an autologous anti-CD19 chimeric antigen receptor (CAR) T cell therapy, approved for the treatment of relapsed/refractory diffuse large B-cell lymphoma (r/r DLBCL) after ≥ 2 prior lines of therapy. T-cell exhaustion due to an immunosuppressive environment has been a hypothesized mechanism for CAR-T cell therapy failure. Subgroup analyses of the JULIET trial suggested an association between programmed cell death 1 (PD-1) and programmed death ligand 1 (PD-L1) interaction in baseline biopsies and lack of response (Agoulnik et al. EHA. 2018). Moreover, the anti-PD-1 monoclonal antibody pembrolizumab has shown clinical activity in r/r DLBCL after failing tisagenlecleucel therapy (Chong et al. Blood. 2017). PORTIA is a phase 1b, multicenter, open-label trial investigating the safety and efficacy of tisagenlecleucel plus pembrolizumab in patients with r/r DLBCL. We report data from a completed cohort of the ongoing study.
Methods: Eligible patients must be ≥ 18 years old with a confirmed diagnosis of DLBCL that has relapsed after or is refractory to ≥ 2 prior lines of therapy and Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. Patients treated with prior allogeneic stem cell transplantation, anti-CD19 therapies, or checkpoint inhibitors are excluded. Lymphodepleting chemotherapy consists of fludarabine-cyclophosphamide. Patients receive a single tisagenlecleucel intravenous infusion (target dose: 0.6-6.0x108 cells) on Day 1. Pembrolizumab is given at 200 mg every 21 days, for up to 6 doses. Pembrolizumab was started on Day 15 post-tisagenlecleucel in Cohort 1, with the option of moving to Day 8 or 22 in subsequent cohorts, based on observed data and guided by a Bayesian Logistic Regression Model with Escalation with Overdose Control principle, evaluating the distribution of dose-limiting toxicities (DLTs) occurring in the 21 days following the first pembrolizumab dose. As per study protocol, a total of 20 patients will be treated at the optimal dose timing. Primary endpoints are the proportion of patients receiving pembrolizumab per protocol schedule, the incidence of DLTs in the dose-timing selection phase, and the overall response rate in the dose-expansion phase. Secondary outcomes include duration of response, progression-free survival, overall survival, safety, cellular kinetics, and immunogenicity.
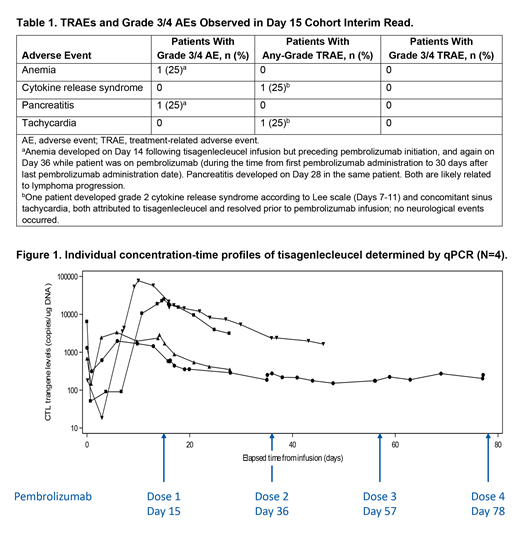
Results: As of 5 March 2019, 5 patients were screened for Cohort 1. Four patients were enrolled and received tisagenlecleucel and pembrolizumab. Median age was 54 (range, 35-79). Median follow-up from time from tisagenlecleucel infusion to data cut-off was 46 days (range, 36-85). Patients received 1.7-3.0x108 CAR-positive T cells, and 1, 2, 2 and 4 pembrolizumab doses, respectively, with no delays. All 4 patients experienced at least 1 adverse event (AE), with no exacerbation or recurrence of tisagenlecleucel-related AEs following pembrolizumab infusion. No pembrolizumab-related AEs were observed. No DLTs or grade 3-4 treatment-related adverse events (TRAEs) were observed. TRAEs and AEs are summarized in Table 1. Two patients discontinued pembrolizumab treatment (after 1 and 2 doses, respectively) due to disease progression. All 4 patients experienced initial expansion between Days 6 and 15 post-tisagenlecleucel infusion, with peak transgene levels ranging from 1,980 to 77,200 copies/µg DNA (Figure 1). No secondary expansion was observed after pembrolizumab administration. The overall exposure is consistent with the observed exposure in r/r DLBCL patients in the JULIET trial. With very limited follow-up, 1 partial response has been observed. Cohort 2 (pembrolizumab starting Day 8) was ongoing at the time of submission.
Conclusions: Overall, PD-1 blockade with pembrolizumab on Day 15 after tisagenlecleucel infusion was feasible and showed a manageable safety profile in the first 4 patients. No DLTs and no clinically significant exacerbation of AEs were observed, supporting the initiation of Cohort 2. Efficacy and safety data with an updated cutoff for Cohort 1 and new data from Cohort 2 will be presented at the congress.
Clinical trial information: NCT03630159.
Jaeger:Novartis, Roche, Sandoz: Consultancy; AbbVie, Celgene, Gilead, Novartis, Roche, Takeda Millennium: Research Funding; Amgen, AbbVie, Celgene, Eisai, Gilead, Janssen, Novartis, Roche, Takeda Millennium, MSD, BMS, Sanofi: Honoraria; Celgene, Roche, Janssen, Gilead, Novartis, MSD, AbbVie, Sanofi: Membership on an entity's Board of Directors or advisory committees. Worel:Sanofi Genzyme, Malinckrodt Therakos: Research Funding; Jazz, Sanofi, Celgene, Novartis, Malinckrodt Therakos: Honoraria; Sanofi Genzyme, Malinckrodt Therakos: Speakers Bureau. McGuirk:Juno Therapeutics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Bellicum Pharmaceuticals: Research Funding; Astellas: Research Funding; Fresenius Biotech: Research Funding; Novartis: Research Funding; ArticulateScience LLC: Other: Assistance with manuscript preparation; Pluristem Ltd: Research Funding; Gamida Cell: Research Funding; Kite Pharmaceuticals: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau. Riedell:Kite/Gilead: Honoraria, Research Funding, Speakers Bureau; Novartis: Research Funding; Verastem: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; Bayer: Honoraria, Speakers Bureau. Fleury:AstraZeneca: Consultancy; Abbvie: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Seattle Genetics: Consultancy, Honoraria; Roche: Consultancy, Honoraria; Gilead: Consultancy, Honoraria; Novartis: Consultancy, Honoraria. Chu:Novartis: Employment. Abdelhady:Novartis: Employment. Forcina:Novartis: Employment. Bubuteishvili Pacaud:Novartis: Employment. Waller:Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Pharmacyclics: Other: Travel expenses, Research Funding; Cerus Corporation: Other: Stock, Patents & Royalties; Chimerix: Other: Stock; Cambium Oncology: Patents & Royalties: Patents, royalties or other intellectual property ; Amgen: Consultancy; Kalytera: Consultancy.

