

Introduction
Extramedullary myeloma (EMM) is the synchronous presence of clonal plasma cells (CPC) in both bone marrow and distant sites. Its frequency is reported among 6-20% of multiple myeloma (MM) patients and can manifest as osseous plasmacytoma (OP) or non-osseous plasmacytoma (NOP). Previous reports outline a more aggressive clinical behavior in patients presenting with EMM and in Latin American population. However, there is scarce data regarding EMM in Latin American patients. The aim of this study was to describe the clinical characteristics and impact of EMM on survival outcomes in all patients diagnosed and followed at our institution.
Methods
Retrospective single-center study that included >18-year-old MM patients, as defined by the IMWG criteria. EMM was defined as the presence of CPC in any osseous or non-osseous tissue outside of the bone marrow or as the demonstration of a synchronous tumor at a non-accessible site by imaging methods.
Results
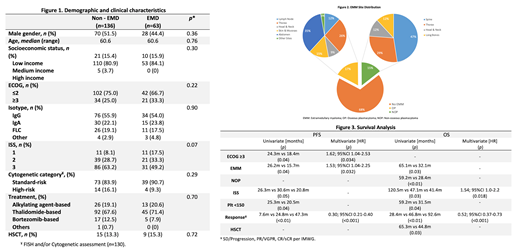
A total of 199 patients were included. Demographic and clinical characteristics are shown in Figure 1. Sixty-three patients had EMM (31.8%), of which 45 cases (71.4%) presented at diagnosis and 18 (28.6%) at progression. Forty-eight cases (76.2%) were diagnosed by biopsy and 15 (23.8%) by imaging studies. Fifty-four percent (n=34) of the cases presented as OP and 46% (n=29) as NOP.
Most-frequently involved sites included the spine and chest wall in OP and abdomen and thorax in NOP (Figure 2). EMM was associated with lower comorbidity rates and higher incidence of renal failure. Mean progression-free survival (PFS) and overall survival (OS) were 22.9 and 43.7 months, respectively. EMM at any time of disease course resulted on lower PFS and OS (15.7 months vs. 26.2 months, p=0.04; 32.1 months vs. 65.1 months, p=0.03). The presence of NOP was related with lower OS (28.4 months vs. 59.2 months, p<0.01). A higher ECOG (HR 1.62; 95%CI 1.04-2.53; p=0.034), less profound responses to treatment (HR 0.30; 95%CI 0.21-0.40; p<0.001), and the presence of EMM (HR 1.53; 95%CI 1.04-2.25; p=0.032) were associated with worse PFS; while both high ISS (HR 1.54; 95%CI 1.0-2.2; p=0.018) and less profound responses (HR 0.52; 95%CI 0.37-0.73; p<0.001) resulted in worse OS in multivariate analysis. Other factors affecting PFS and OS are shown in Figure 3.
Conclusion
We observed higher rates of EMM in our cohort when compared with the reported literature. The presence of EMM was associated with poor prognosis as evidenced by lower PFS and OS. When comparing OP vs. NOP EMM, NOP conferred an increased risk of early mortality. Results suggest that more aggressive disease biology, higher tumor burden, and/or delayed referral for diagnosis and therapy in our population of MM patients contribute to these unfavorable outcomes.
It is imperative that our knowledge on high-risk MM groups, including EMM, in minorities is expanded. Latin American countries are urged to work together in collaborative research to confirm these results in order to properly identify patients who may benefit from more intensive treatment that might result in the improvement of long-term outcomes.
Martinez-Banos:Celgene, Amgen: Other: Advisory Board.

