

INTRODUCTION
Only half of the patients with gut predominant acute graft-versus-host disease (aGvHD) respond to first-line treatment (corticosteroids). No consensus has yet been reached on treatment in the second and subsequent lines. There are several case reports supporting the role of fecal microbiota transplantation (FMT) in the treatment of steroid-resistant GvHD. Here we present the results of FMT in one of the largest cohorts of patients with acute (a) and chronic (c) GvHD, mostly with gut manifestation.
MATERIAL AND METHODS
12 patients aged 26-67 years underwent a total of 15 FMTs to decolonize the gastrointestinal tract (GI) from antibiotic-resistant bacteria (ARB). In all of them steroid resistant GvHD (2 patients with cGvHD and 10 with aGvHD) coexisted. All patients with aGvHD had GI tract involvement (median grade: 3), 7 had skin (median grade: 3) and 5 had liver (median grade: 1) GvHD symptoms. Patients with cGvHD presented progressive involvement of the skin, lungs, pericardium and eyes. FMT was performed as two infusions by nasoduodenal tube of a 100g/200 ml solution of feces, on following days.
OUTCOMES
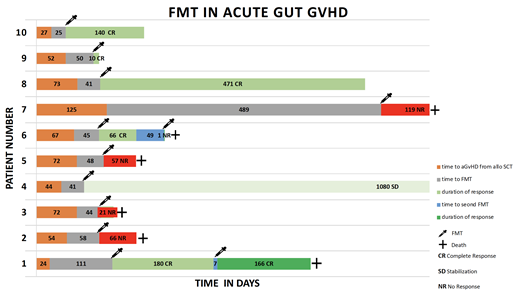
The median time from aGvHD diagnosis to the first FMT treatment was 46.5 days (8-489 days). Most patients were still on steroids during FMT (median dose 0.5 mg metyloprednisolone/kg of body weight). As a result, in 10/12 patients (83%) ARB decolonization was observed. Overall response rate (ORR) in the case of aGvHD reached 58% (7/12 performed FMTs), including CR in 4/12 (33%) cases. Median duration of response to relapse or death was 168 days (10-1080 days). The majority of patients who responded to FMT (5/6, 83%) underwent the procedure in a better general condition (ECOG≤2). Severe general condition (ECOG> 2) seemed to be related with the presence of serious complications after FMT. Both patients with cGvHD achieved stabilization or improvement of organ disease, which may be related with FMT procedure (there is no data on use FMT in cGvHD).
COMPLICATIONS
Among the complications of FMT with a possible cause-effect relationship there were: 1 death in close relation with FMT (respiratory failure in the course of pneumonia), 3 septic episodes, 2 subileus episodes and one case of diarrhea. In the latter case, the workup revealed norovirus infection originating from the fecal material of the donor (who was asymptomatic).
CONCLUSIONS
The described results indicate that FMT may be an effective treatment option for severe GvH disease. Patients undergoing the procedure should be qualified early enough to avoid life-threatening complications and maximize the likelihood of responding to treatment.
Jedrzejczak:Amgen: Consultancy, Other: travel support for hematology meetings (ASH, EBMT, EHA) ; Celgene: Other: travel support for hematology meetings (ASH, EBMT, EHA) ; Takeda: Consultancy; Novartis: Research Funding; Roche: Other: travel support for hematology meetings (ASH, EBMT, EHA) . Basak:Teva: Honoraria; Celgene: Honoraria.

