

Introduction. Children with sickle cell anemia enrolled in Realizing Effectiveness Across Continents with Hydroxyurea (REACH, NCT01966731) received open-label hydroxyurea at maximum tolerated dose (MTD) in four countries within sub-Saharan Africa (Tshilolo et al, NEJM 2019;380:121-131). Unlike children in the United States or Europe, a substantial proportion of REACH participants had splenomegaly at enrollment, and more developed splenomegaly while receiving hydroxyurea. Splenic enlargement in association with hydroxyurea treatment in sub-Saharan Africa is previously unrecognized, and its causes and consequences remain unclear.
Methods. Palpable splenomegaly was evaluated at both the mid-clavicular and mid-axillary lines at each scheduled and unscheduled sick visit. The size of the spleen, defined as the greatest distance (cm) below the subcostal margin, was recorded in the REDCap trial database at all four clinical sites. Cross-sectional analysis was performed at baseline enrollment using four spleen categories (Not Palpable, 1-4 cm, ≥5 cm, or Splenectomy) with correlations for age, sex, site, growth parameters, alpha-thalassemia trait and G6PD deficiency. This analysis was repeated using the largest spleen size over the first two years on hydroxyurea, but examining two-year laboratory values and also the hydroxyurea dose at MTD, time to MTD, dose-limiting toxicities, and clinical outcomes including acute splenic sequestration, malaria infections, and sepsis.
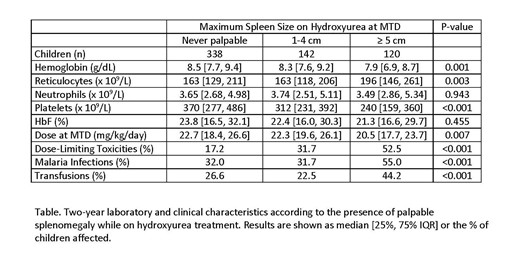
Results. A total of 606 children started hydroxyurea study treatment, including 6 (1.0%) with previous splenectomy, 59 (9.7%) with previous splenic sequestration, and 99 (16.3%) with palpable splenomegaly at enrollment (52 children with 1-4 cm and 47 with ≥5 cm). Large spleens (≥5 cm) were commonly observed at baseline at all clinical sites except Uganda, which identified only 1 child. Compared to those with no palpable spleen, children with large spleens at baseline had similar age and growth parameters, but were significantly more likely to have alpha-thalassemia (78.7% versus 56.2%, P=0.004) and also G6PD deficiency among males (28.0% versus 17.6%, P=0.32). Children with large spleens at enrollment also had a lower hemoglobin (Hb = 6.5 versus 7.3 g/dL, P<0.001) and lower platelet count (platelets = 227 versus 410 x 109/L, P<0.001), but equivalent fetal hemoglobin (HbF = 10.2 versus 9.4%, P=0.82). On hydroxyurea treatment with escalation to MTD, 262 children (43.7%) had palpable splenomegaly recorded, including 120 (20.0%) with spleens ≥5 cm. These large spleens were observed at all four clinical sites, with DRC having the most (52) and Uganda with the least (14). After 24 months of hydroxyurea treatment, laboratory differences were noted according to the cumulative occurrence of splenomegaly including a significantly lower hemoglobin and platelet count, higher absolute reticulocyte count, and lower hydroxyurea dose at MTD (Table). Large spleens were associated with a high cumulative incidence of laboratory dose-limiting toxicities, as well as a significantly higher risk of having clinically symptomatic malaria and receiving blood transfusions (Table). A total of 31 children (5.2%) on hydroxyurea treatment received elective splenectomy, including one partial splenectomy using arterial embolization.
Conclusion. Children with sickle cell anemia living in sub-Saharan Africa have an increased risk of having palpable splenomegaly, which is further increased while receiving hydroxyurea treatment. Large spleen at baseline were associated with lower blood counts, consistent with hypersplenism. On hydroxyurea treatment, children with large spleens had significantly lower blood counts and more dose-limiting toxicities, which lowered their eventual hydroxyurea dose at MTD but still led to robust HbF responses. Children with large spleens were also at higher risk of developing malaria infections, receiving transfusions, and requiring surgical splenectomy. Splenic enlargement in association with hydroxyurea treatment was common in children with sickle cell anemia in the REACH trial; its cause remains unclear but the consequences include substantial laboratory toxicity and clinical morbidity. Investigating the etiologies and management of children with chronically enlarged spleens is crucial before expanding hydroxyurea access across Africa for sickle cell anemia.
Ware:Global Blood Therapeutics: Membership on an entity's Board of Directors or advisory committees; Bristol Myers Squibb: Other: Research Drug Donation; Nova Laboratories: Membership on an entity's Board of Directors or advisory committees; CSL Behring: Membership on an entity's Board of Directors or advisory committees; Novartis: Other: DSMB; Agios: Membership on an entity's Board of Directors or advisory committees; Addmedica: Other: Research Drug Donation.

